Lancet. 2019 Sep 28;394(10204):1159-1168. doi: 10.1016/S0140-6736(19)31709-X. Epub 2019 Aug 29.
Published findings on breast cancer risk associated with different types of menopausal hormone therapy (MHT) are inconsistent, with limited information on long-term effects. We bring together the epidemiological evidence, published and unpublished, on these associations, and review the relevant randomised evidence.
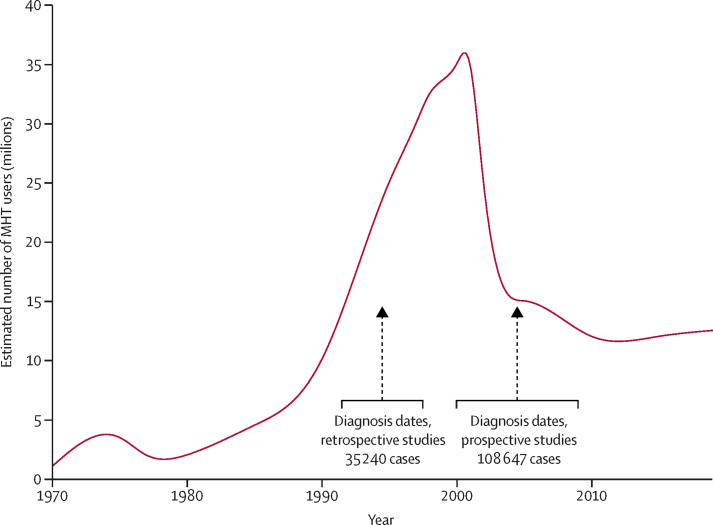
Principal analyses used individual participant data from all eligible prospective studies that had sought information on the type and timing of MHT use; the main analyses are of individuals with complete information on this. Studies were identified by searching many formal and informal sources regularly from Jan 1, 1992, to Jan 1, 2018. Current users were included up to 5 years (mean 1·4 years) after last-reported MHT use. Logistic regression yielded adjusted risk ratios (RRs) comparing particular groups of MHT users versus never users.
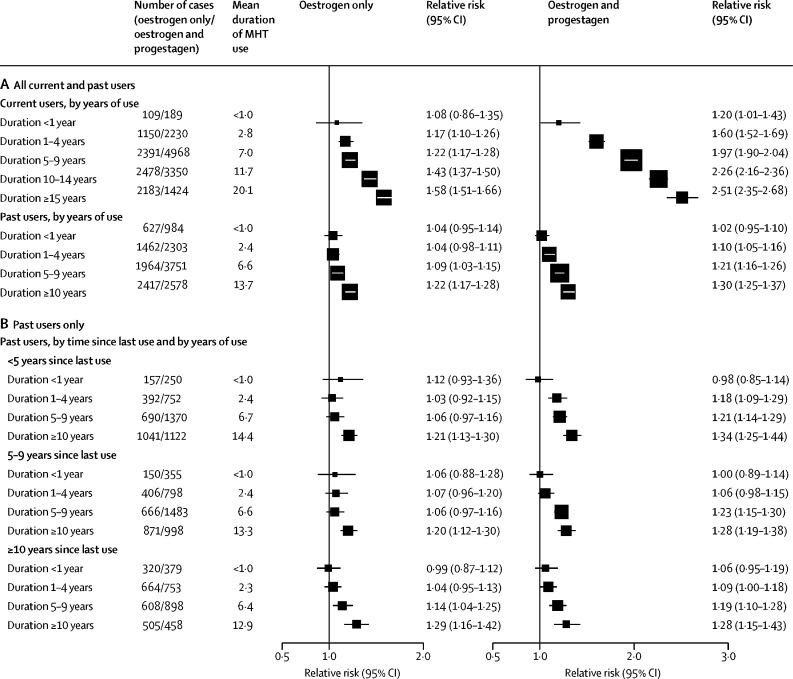
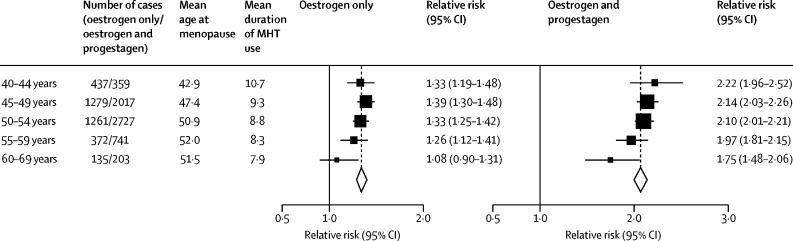
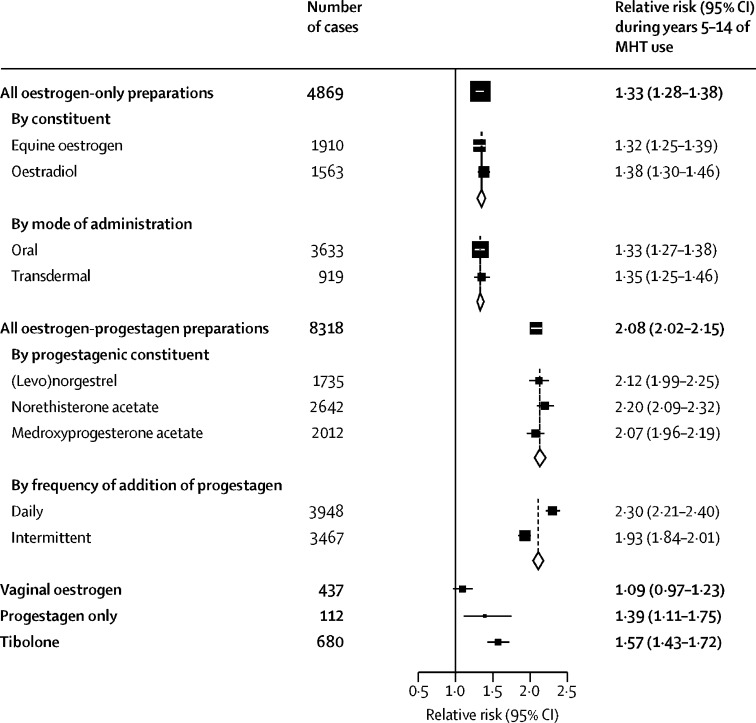
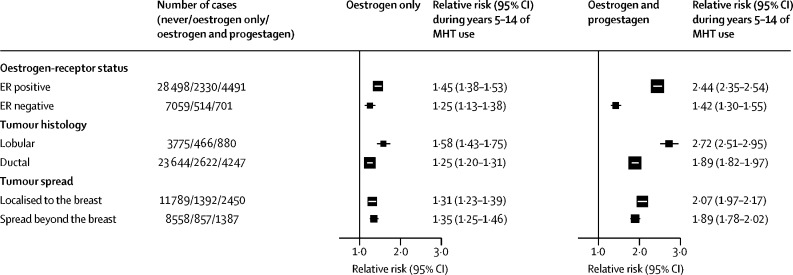
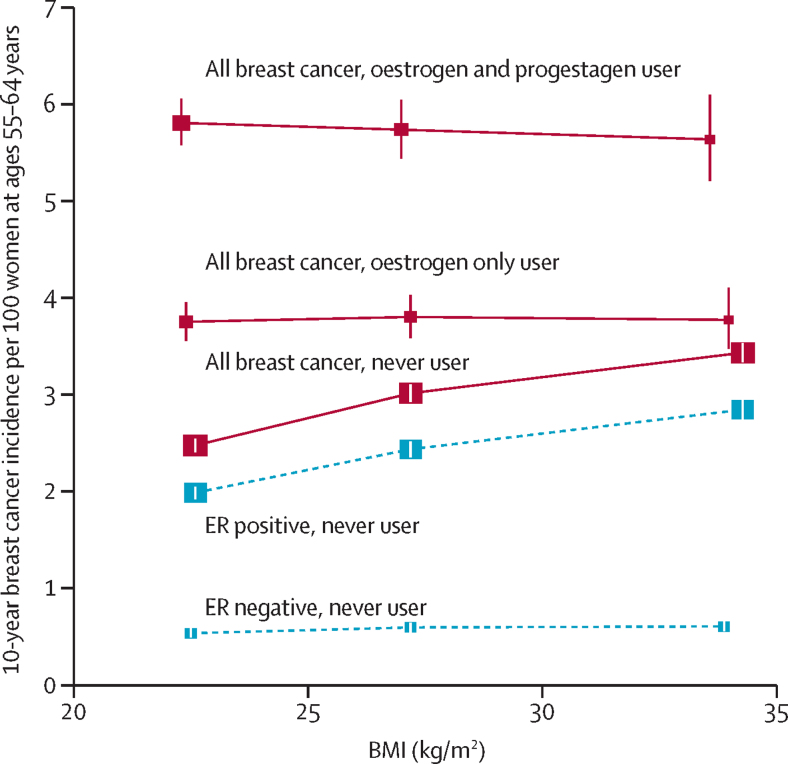
During prospective follow-up, 108 647 postmenopausal women developed breast cancer at mean age 65 years (SD 7); 55 575 (51%) had used MHT. Among women with complete information, mean MHT duration was 10 years (SD 6) in current users and 7 years (SD 6) in past users, and mean age was 50 years (SD 5) at menopause and 50 years (SD 6) at starting MHT. Every MHT type, except vaginal oestrogens, was associated with excess breast cancer risks, which increased steadily with duration of use and were greater for oestrogen-progestagen than oestrogen-only preparations. Among current users, these excess risks were definite even during years 1-4 (oestrogen-progestagen RR 1·60, 95% CI 1·52-1·69; oestrogen-only RR 1·17, 1·10-1·26), and were twice as great during years 5-14 (oestrogen-progestagen RR 2·08, 2·02-2·15; oestrogen-only RR 1·33, 1·28-1·37). The oestrogen-progestagen risks during years 5-14 were greater with daily than with less frequent progestagen use (RR 2·30, 2·21-2·40 vs 1·93, 1·84-2·01; heterogeneity p<0·0001). For a given preparation, the RRs during years 5-14 of current use were much greater for oestrogen-receptor-positive tumours than for oestrogen-receptor-negative tumours, were similar for women starting MHT at ages 40-44, 45-49, 50-54, and 55-59 years, and were attenuated by starting after age 60 years or by adiposity (with little risk from oestrogen-only MHT in women who were obese). After ceasing MHT, some excess risk persisted for more than 10 years; its magnitude depended on the duration of previous use, with little excess following less than 1 year of MHT use.
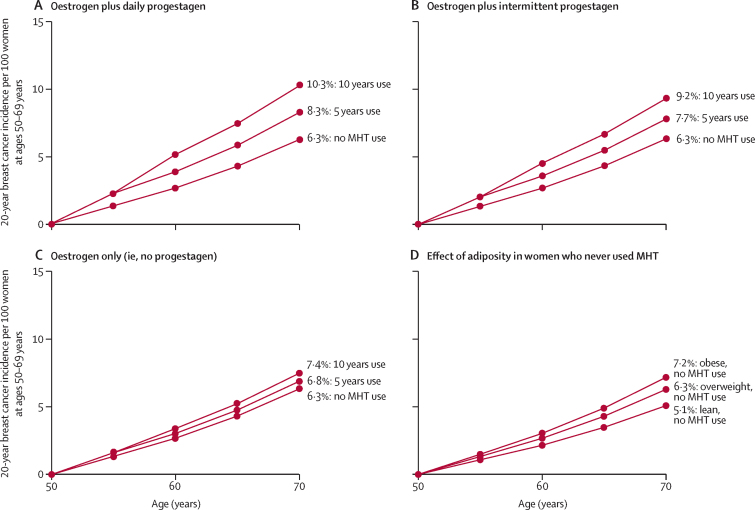
If these associations are largely causal, then for women of average weight in developed countries, 5 years of MHT, starting at age 50 years, would increase breast cancer incidence at ages 50-69 years by about one in every 50 users of oestrogen plus daily progestagen preparations; one in every 70 users of oestrogen plus intermittent progestagen preparations; and one in every 200 users of oestrogen-only preparations. The corresponding excesses from 10 years of MHT would be about twice as great.
Cancer Research UK and the Medical Research Council.
关于不同类型的绝经激素治疗(MHT)与乳腺癌风险之间的关联,已发表的研究结果并不一致,且有关长期影响的信息有限。我们汇集了这些关联的流行病学证据,包括已发表和未发表的研究,并对相关的随机对照试验进行了综述。
主要分析使用了所有有资格的前瞻性研究的个体参与者数据,这些研究都寻求了关于 MHT 使用类型和时机的信息;主要分析是基于对这些信息完整的个体。通过定期从 1992 年 1 月 1 日至 2018 年 1 月 1 日搜索许多正式和非正式的来源来确定研究。当前使用者的纳入时间截止到最后一次报告 MHT 使用后的 5 年内(平均 1.4 年)。逻辑回归产生了比较特定 MHT 使用者与从不使用者的调整后风险比(RR)。
在前瞻性随访期间,108647 名绝经后女性在平均年龄 65 岁(标准差 7)时患上乳腺癌;55575 名(51%)曾使用过 MHT。在有完整信息的女性中,当前使用者的 MHT 持续时间平均为 10 年(标准差 6),过去使用者为 7 年(标准差 6),绝经时的平均年龄为 50 岁(标准差 5),开始使用 MHT 时为 50 岁(标准差 6)。除阴道雌激素外,每种 MHT 类型都与乳腺癌风险增加有关,且这种风险随使用时间的延长而稳步增加,雌激素-孕激素制剂的风险大于雌激素制剂。在当前使用者中,即使在 1-4 年内(雌激素-孕激素 RR 1.60,95%CI 1.52-1.69;雌激素制剂 RR 1.17,1.10-1.26),这些额外风险也非常明确,在 5-14 年内,风险增加了一倍(雌激素-孕激素 RR 2.08,2.02-2.15;雌激素制剂 RR 1.33,1.28-1.37)。在 5-14 年内,与使用较不频繁的孕激素相比,每日使用孕激素与雌激素-孕激素制剂的风险增加(RR 2.30,2.21-2.40 与 1.93,1.84-2.01;异质性 p<0.0001)。对于特定的制剂,在 5-14 年内当前使用者的 RR 对于雌激素受体阳性肿瘤比对于雌激素受体阴性肿瘤大得多,对于在 40-44 岁、45-49 岁、50-54 岁和 55-59 岁开始使用 MHT 的女性相似,并且在 60 岁以后开始使用或肥胖(对于肥胖的女性,雌激素单独使用 MHT 的风险较小)会减弱。停止 MHT 后,超过 10 年仍存在一些额外的风险;其大小取决于先前使用的时间长短,MHT 使用时间少于 1 年,风险增加较小。
如果这些关联主要是因果关系,那么对于发达国家平均体重的女性,如果在 50 岁时开始使用 5 年的 MHT,那么在 50-69 岁年龄组中,雌激素加每日孕激素制剂的使用者每 50 人就会增加一例乳腺癌;雌激素加间歇性孕激素制剂的使用者每 70 人会增加一例;雌激素制剂的使用者每 200 人会增加一例。如果使用 10 年 MHT,这种额外的风险会增加一倍左右。
英国癌症研究中心和医学研究委员会。