Orimoloye Olusola A, Banga Sandeep, Dardari Zeina A, Uddin S M Iftekhar, Budoff Matthew J, Berman Daniel S, Rozanski Alan, Shaw Leslee J, Rumberger John A, Nasir Khurram, Miedema Michael D, Blumenthal Roger S, Blaha Michael J, Mirbolouk Mohammadhassan
Johns Hopkins Ciccarone Center for the Prevention of Cardiovascular Disease, Johns Hopkins School of Medicine, Baltimore, Maryland.
Department of Medicine, University of Illinois College of Medicine at Peoria, Peoria, Illinois.
Coron Artery Dis. 2019 Dec;30(8):608-614. doi: 10.1097/MCA.0000000000000746.
Coronary artery calcium (CAC) has been shown in multiple populations to predict atherosclerotic cardiovascular disease. However, its predictive value in Asian-Americans is poorly described.
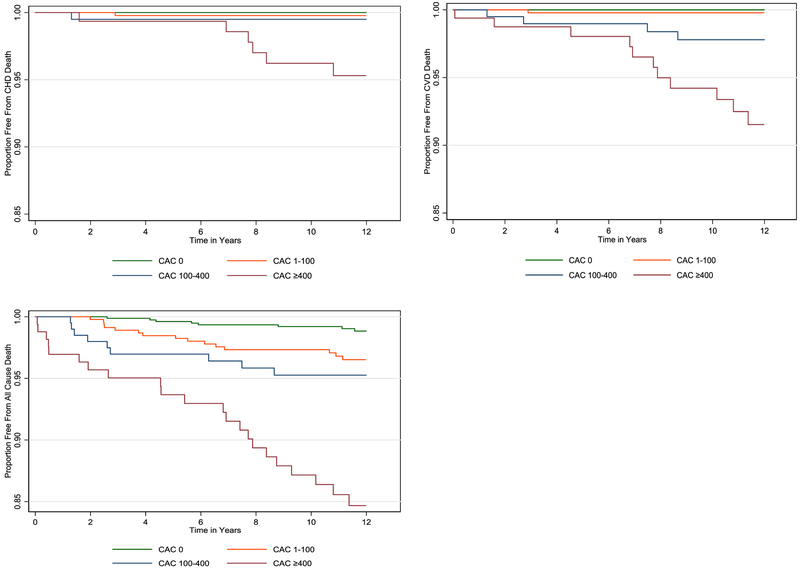
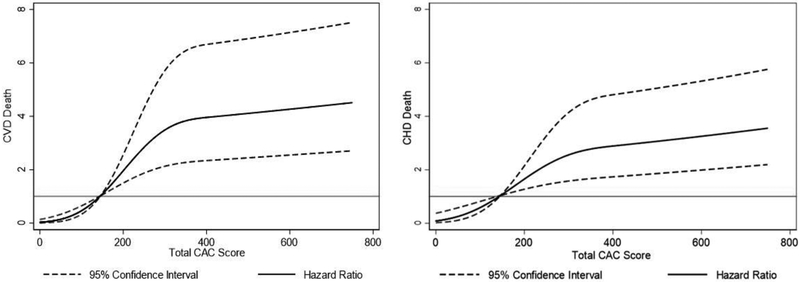
We studied 1621 asymptomatic Asian-Americans in the CAC Consortium, a large multicenter retrospective cohort. CAC was modeled in categorical (CAC = 0; CAC = 1-99; CAC = 100-399; CAC ≥ 400) and continuous [ln (CAC + 1)] forms. Participants were followed over a mean follow-up of 12 ± 4 years for coronary heart disease (CHD) death, cardiovascular disease (CVD) death, and all-cause mortality. The predictive value of CAC for individual outcomes was assessed using multivariable-adjusted Cox regression models adjusted for traditional cardiovascular risk factors and reported as hazard ratios (95% confidence interval).
The mean (SD) age of the population was 54 (11.2) years and 64% were men. The mean 10-year atherosclerotic cardiovascular disease risk score was 8%. Approximately half had a CAC score of 0, whereas 22.5% had a CAC score of greater than 100. A total of 56 deaths (16 CVD and 8 CHD) were recorded, with no CVD or CHD deaths in the CAC = 0 group. We noted a significantly increased risk of CHD [hazard ratio (HR): 2.6 (1.5-4.3)] and CVD [HR: 2.3 (1.8-2.9)] mortality per unit increase in In (CAC + 1). Compared to those with CAC scores of 0, individuals with CAC scores of at least 400 had over a three-fold increased risk of all-cause mortality [HR: 3.3 (1.3-8.6)].
Although Asian-Americans are a relatively low-risk group, CAC strongly predicts CHD, CVD, and all-cause mortality beyond traditional risk factors. These findings may help address existing knowledge gaps in CVD risk prediction in Asian-Americans.
在多个人群中,冠状动脉钙化(CAC)已被证明可预测动脉粥样硬化性心血管疾病。然而,其在亚裔美国人中的预测价值描述甚少。
我们在CAC联盟中研究了1621名无症状亚裔美国人,这是一个大型多中心回顾性队列。CAC以分类形式(CAC = 0;CAC = 1 - 99;CAC = 100 - 399;CAC≥400)和连续形式[ln(CAC + 1)]进行建模。对参与者进行了平均12±4年的随访,观察冠心病(CHD)死亡、心血管疾病(CVD)死亡和全因死亡率。使用针对传统心血管危险因素进行多变量调整的Cox回归模型评估CAC对个体结局的预测价值,并报告为风险比(95%置信区间)。
该人群的平均(标准差)年龄为54(11.2)岁,64%为男性。平均10年动脉粥样硬化性心血管疾病风险评分为8%。约一半人的CAC评分为0,而22.5%的人CAC评分大于100。共记录了56例死亡(16例CVD和8例CHD),在CAC = 0组中无CVD或CHD死亡。我们注意到ln(CAC + 1)每增加一个单位,CHD[风险比(HR):2.6(1.5 - 4.3)]和CVD[HR:2.3(1.8 - 2.9)]死亡率显著增加。与CAC评分为0的人相比,CAC评分至少为400的人全因死亡率风险增加了三倍多[HR:3.3(1.3 - 8.6)]。
尽管亚裔美国人是相对低风险群体,但CAC强烈预测CHD、CVD和全因死亡率,超出了传统危险因素。这些发现可能有助于填补亚裔美国人CVD风险预测方面现有的知识空白。