Forbang Nketi I, Michos Erin D, McClelland Robyn L, Remigio-Baker Rosemay A, Allison Matthew A, Sandfort Veit, Ix Joachim H, Thomas Isac, Rifkin Dena E, Criqui Michael H
From the Department of Family Medicine and Public Health, University of California, San Diego, La Jolla (N.I.F., R.A.R.-B., M.A.A., J.H.I., I.T., D.E.R., M.H.C.); Department of Medicine, Johns Hopkins University, Baltimore, MD (E.D.M.); Department of Biostatistics, University of Washington, Seattle (R.L.M.); Veterans Administration San Diego Healthcare System, La Jolla, CA (M.A.A., J.H.I., D.E.R.); and Clinical Center, National Institutes of Health, Bethesda, MD (V.S.).
Circ Cardiovasc Imaging. 2016 Nov;9(11). doi: 10.1161/CIRCIMAGING.116.005138.
Abdominal aortic calcium (AAC) and coronary artery calcium (CAC) independently and similarly predict cardiovascular disease (CVD) events. The standard AAC and CAC score, the Agatston method, upweights for greater calcium density, thereby modeling higher calcium density as a CVD hazard.
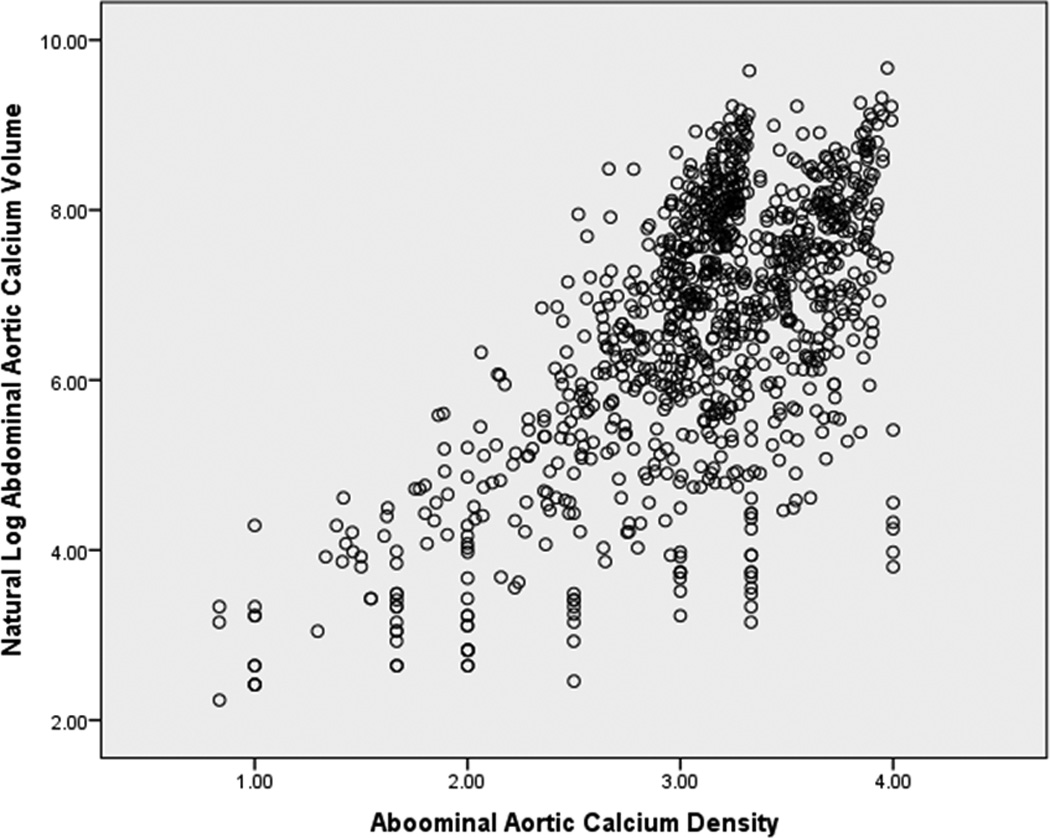
Computed tomography scans were used to measure AAC and CAC volume and density in a multiethnic cohort of community-dwelling individuals, and Cox proportional hazard was used to determine their independent association with incident coronary heart disease (CHD, defined as myocardial infarction, resuscitated cardiac arrest, or CHD death), cardiovascular disease (CVD, defined as CHD plus stroke and stroke death), and all-cause mortality. In 997 participants with Agatston AAC and CAC scores >0, the mean age was 66±9 years, and 58% were men. During an average follow-up of 9 years, there were 77 CHD, 118 CVD, and 169 all-cause mortality events. In mutually adjusted models, additionally adjusted for CVD risk factors, an increase in ln(AAC volume) per standard deviation was significantly associated with increased all-cause mortality (hazard ratio=1.20; 95% confidence interval, 1.08-1.33; P<0.01) and an increased ln(CAC volume) per standard deviation was significantly associated with CHD (hazard ratio=1.17; 95% confidence interval, 1.04-1.59; P=0.02) and CVD (hazard ratio=1.20; 95% confidence interval, 1.05-1.36; P<0.01). In contrast, both AAC and CAC density were not significantly associated with CVD events.
The Agatston method of upweighting calcium scores for greater density may be inappropriate for CVD risk prediction in both the abdominal aorta and coronary arteries.
腹主动脉钙化(AAC)和冠状动脉钙化(CAC)可独立且相似地预测心血管疾病(CVD)事件。标准的AAC和CAC评分方法,即阿加斯顿法,对更高的钙密度赋予更高权重,从而将更高的钙密度建模为心血管疾病风险。
使用计算机断层扫描测量多民族社区居住个体队列中的AAC和CAC体积及密度,并采用Cox比例风险模型确定它们与冠心病(CHD,定义为心肌梗死、心脏骤停复苏或CHD死亡)、心血管疾病(CVD,定义为CHD加中风及中风死亡)和全因死亡率的独立关联。在997名阿加斯顿AAC和CAC评分>0的参与者中,平均年龄为66±9岁,58%为男性。在平均9年的随访期间,发生了77例CHD、118例CVD和169例全因死亡事件。在相互调整的模型中,进一步调整了CVD危险因素,每标准差的ln(AAC体积)增加与全因死亡率增加显著相关(风险比=1.20;95%置信区间,1.08 - 1.33;P<0.01),每标准差的ln(CAC体积)增加与CHD(风险比=1.17;95%置信区间,1.04 - 1.59;P = 0.02)和CVD(风险比=1.20;95%置信区间,1.05 - 1.36;P<0.01)显著相关。相比之下,AAC和CAC密度均与CVD事件无显著关联。
阿加斯顿法对更高密度的钙评分赋予更高权重,可能不适用于腹主动脉和冠状动脉的CVD风险预测。