CAPRISA-Centre for the AIDS Programme of Research in South Africa, University of KwaZulu-Natal, Private Bag X7, Congella, Durban, 4013, South Africa.
MRC-CAPRISA HIV-TB Pathogenesis and Treatment, Research Unit, Nelson R Mandela School of Medicine, Doris Duke Medical Research Institute (2nd floor), University of KwaZulu-Natal, 719 Umbilo Road, Private Bag X7, Congella, Durban, 4013, South Africa.
BMC Infect Dis. 2019 Sep 5;19(1):775. doi: 10.1186/s12879-019-4410-8.
South Africa has the highest HIV prevalence and supports the largest antiretroviral therapy (ART) programme globally. With the introduction of a test and treat policy, ensuring long term optimal adherence to ART (≥95%) is essential for successful patient and public health outcomes. The aim of this study was to assess long-term ART adherence to inform best practices for chronic HIV care.
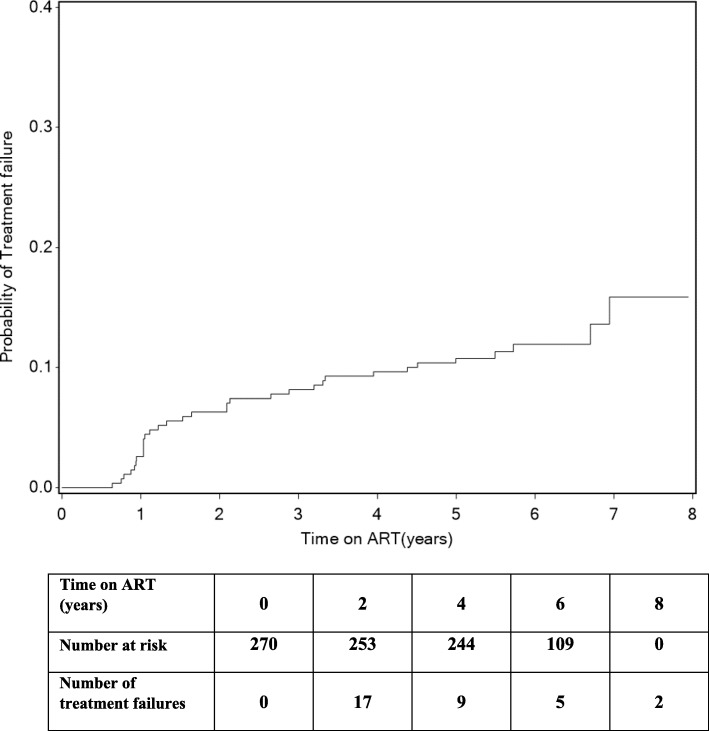
Long-term ART adherence was retrospectively analysed over a median duration of 5 years (interquartile range [IQR]: 5.3-6.5) in patients initially enrolled in a randomised controlled trial assessing tuberculosis and HIV treatment integration and subsequently followed post-trial in an observational cohort study in Durban, South Africa. The association between baseline patient characteristics and adherence over time was estimated using generalized estimating equations (GEE). Adherence was assessed using pharmacy pill counts conducted at each study visit and compared to 6 monthly viral load measurements. A Kaplan Meier survival analysis was used to estimate time to treatment failure. The McNemar test (with exact p-values) was used to determine the effect of pill burden and concurrent ART and tuberculosis treatment on adherence.
Of the 270 patients included in the analysis; 54.8% were female, median age was 34 years (IQR:29-40) and median time on ART was 70 months (IQR = 64-78). Mean adherence was ≥95% for each year on ART. Stable patients provided with an extended 3-month ART supply maintained adherence > 99%. At study end, 96 and 94% of patients were optimally adherent and virologically suppressed, respectively. Time since ART initiation, female gender and primary breadwinner status were significantly associated with ≥95% adherence to ART. The cumulative probability of treatment failure was 10.7% at 5 years after ART initiation. Concurrent ART and tuberculosis treatment, or switching to a second line ART regimen with higher pill burden, did not impair ART adherence.
Optimal long-term adherence with successful treatment outcomes are possible within a structured ART programme with close adherence monitoring. This adherence support approach is relevant to a resource limited setting adopting a test and treat strategy.
南非拥有最高的艾滋病毒感染率,并在全球范围内支持最大的抗逆转录病毒疗法(ART)计划。随着检测和治疗政策的引入,确保长期(≥95%)最佳的 ART 依从性对于成功的患者和公共卫生结果至关重要。本研究旨在评估长期 ART 依从性,为慢性 HIV 护理提供最佳实践信息。
在南非德班,对最初参加评估结核病和 HIV 治疗整合的随机对照试验的患者进行了中位时间为 5 年(四分位距 [IQR]:5.3-6.5)的长期 ART 依从性回顾性分析,随后在观察性队列研究中进行了随访。使用广义估计方程(GEE)评估基线患者特征与随时间的依从性之间的关系。通过每次研究就诊时进行的药房药丸计数来评估依从性,并与每 6 个月进行的病毒载量测量进行比较。使用 Kaplan-Meier 生存分析来估计治疗失败的时间。使用 McNemar 检验(具有确切的 p 值)来确定药丸负担以及同时进行的 ART 和结核病治疗对依从性的影响。
在纳入分析的 270 例患者中;54.8%为女性,中位年龄为 34 岁(IQR:29-40),中位 ART 治疗时间为 70 个月(IQR=64-78)。每年的 ART 治疗依从性均≥95%。稳定的患者提供了延长的 3 个月 ART 供应,保持了>99%的依从性。研究结束时,96%和 94%的患者分别实现了最佳依从性和病毒学抑制。自开始 ART 治疗以来的时间、女性性别和主要经济来源状态与 ART 依从性≥95%显著相关。ART 治疗开始后 5 年,治疗失败的累积概率为 10.7%。同时进行的 ART 和结核病治疗,或改用具有更高药丸负担的二线 ART 方案,并不会损害 ART 依从性。
在具有密切依从性监测的结构化 ART 计划中,可以实现最佳的长期依从性和成功的治疗结果。这种依从性支持方法与采用检测和治疗策略的资源有限的环境相关。