Centre for Infectious Disease Epidemiology and Research, School of Public Health and Family Medicine, University of Cape Town, Cape Town, South Africa.
Khayelitsha ART Programme and Médecins Sans Frontières, Cape Town, South Africa.
J Int AIDS Soc. 2020 May;23(5):e25476. doi: 10.1002/jia2.25476.
In South Africa, an estimated 4.6 million people were accessing antiretroviral therapy (ART) in 2018. As universal Test and Treat is implemented, these numbers will continue to increase. Given the need for lifelong care for millions of individuals, differentiated service delivery models for ART services such as adherence clubs (ACs) for stable patients are required. In this study, we describe long-term virologic outcomes of patients who have ever entered ACs in Khayelitsha, Cape Town.
We included adult patients enrolled in ACs in Khayelitsha between January 2011 and December 2016 with a recorded viral load (VL) before enrolment. Risk factors for an elevated VL (VL >1000 copies/mL) and confirmed virologic failure (two consecutive VLs >1000 copies/mL one year apart) were estimated using Cox proportional hazards models. VL completeness over time was assessed.
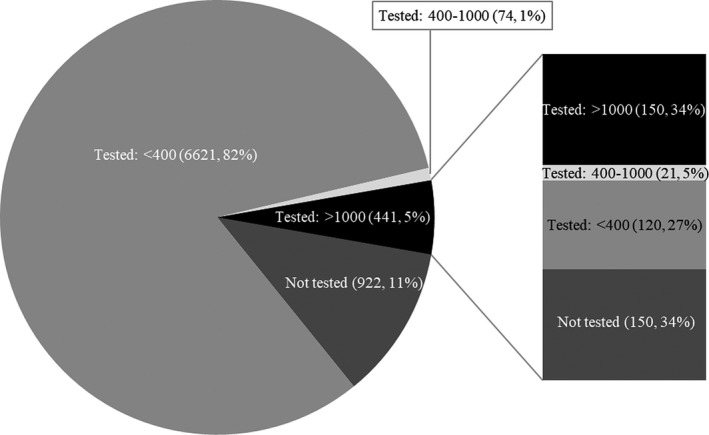
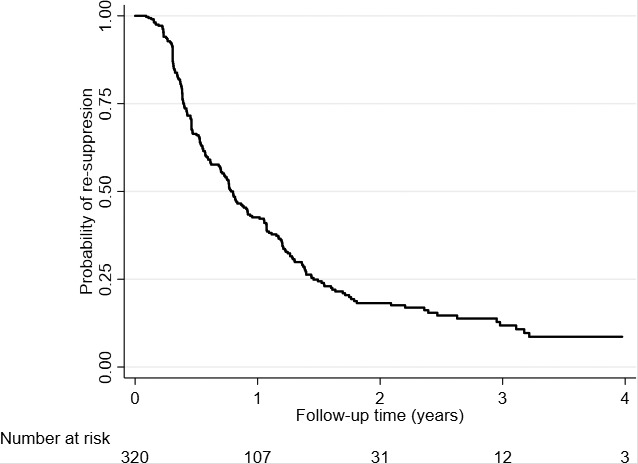
Overall, 8058 patients were included in the analysis, contributing 16,047 person-years of follow-up from AC entry (median follow-up time 1.7 years, interquartile range [IQR]:0.9 to 2.9). At AC entry, 74% were female, 46% were aged between 35 and 44 years, and the median duration on ART was 4.8 years (IQR: 3.0 to 7.2). Among patients virologically suppressed at AC entry (n = 8058), 7136 (89%) had a subsequent VL test, of which 441 (6%) experienced an elevated VL (median time from AC entry 363 days, IQR: 170 to 728). Older age (adjusted hazard ratio [aHR] 0.64, 95% confidence interval [CI] 0.46 to 0.88), more recent year of AC entry (aHR 0.76, 95% CI 0.68 to 0.84) and higher CD4 count (aHR 0.67, 95% CI 0.54 to 0.84) were protective against experiencing an elevated VL. Among patients with an elevated VL, 52% (150/291) with a repeat VL test subsequently experienced confirmed virologic failure in a median time of 112 days (IQR: 56 to 168). Frequency of VL testing was constant over time (82 to 85%), with over 90% of patients remaining virologically suppressed.
This study demonstrates low prevalence of elevated VLs and confirmed virologic failure among patients who entered ACs. Although ACs were expanded rapidly, most patients were well monitored and remained stable, supporting the continued rollout of this model.
在南非,据估计,2018 年有 460 万人接受抗逆转录病毒治疗(ART)。随着普遍检测和治疗的实施,这一数字将继续增加。鉴于数百万人需要终身护理,需要为 ART 服务提供差异化的服务提供模式,例如为稳定患者提供的坚持俱乐部(AC)。在这项研究中,我们描述了在开普敦 Khayelitsha 参加过 AC 的患者的长期病毒学结果。
我们纳入了 2011 年 1 月至 2016 年 12 月期间在 Khayelitsha 参加 AC 的成年患者,他们在登记前有记录的病毒载量(VL)。使用 Cox 比例风险模型估计 VL 升高(VL>1000 拷贝/mL)和确认病毒学失败(两次连续 VL>1000 拷贝/mL,相隔一年)的风险因素。评估了随时间推移的 VL 完整性。
总体而言,共有 8058 名患者纳入分析,从 AC 进入开始,共随访 16047 人年(中位随访时间为 1.7 年,四分位距 [IQR]:0.9 至 2.9)。在 AC 进入时,74%为女性,46%年龄在 35 至 44 岁之间,ART 的中位持续时间为 4.8 年(IQR:3.0 至 7.2)。在 AC 进入时病毒学抑制的患者中(n=8058),7136 名(89%)进行了后续 VL 检测,其中 441 名(6%)出现 VL 升高(中位 AC 进入时间为 363 天,IQR:170 至 728)。年龄较大(调整后的危险比 [aHR] 0.64,95%置信区间 [CI] 0.46 至 0.88)、较近的 AC 进入年份(aHR 0.76,95%CI 0.68 至 0.84)和较高的 CD4 计数(aHR 0.67,95%CI 0.54 至 0.84)是降低 VL 升高风险的保护因素。在出现 VL 升高的患者中,52%(150/291)有重复 VL 检测的患者在中位时间 112 天(IQR:56 至 168)后出现确认的病毒学失败。VL 检测的频率随时间保持不变(82%至 85%),超过 90%的患者仍保持病毒学抑制。
这项研究表明,进入 AC 的患者 VL 升高和确认的病毒学失败的发生率较低。尽管 AC 迅速扩大,但大多数患者得到了很好的监测和稳定,支持继续推出这种模式。