Department of Emergency and Critical Care Medicine, Nippon Medical School Tama Nagayama Hospital, 1-7-1 Nagayama, Tama-shi, Tokyo, 2068512, Japan.
Department of Clinical Epidemiology and Health Economics, School of Public Health, The University of Tokyo, 7-3-1 Hongo, Bunkyo-ku, Tokyo, 1130033, Japan.
J Orthop Surg Res. 2019 Sep 5;14(1):302. doi: 10.1186/s13018-019-1341-4.
The management of cervical spinal cord injury (SCI) has changed drastically in the last decades, and surgery is the primary treatment. However, the optimum timing of early surgical treatment (within 24 h or 72 h after injury) is still controversial. We sought to determine the optimum timing of surgery for cervical SCI, comparing the length of the intensive care unit (ICU) stay and in-hospital mortality in patients who underwent surgical treatments (decompression and stabilization) for cervical SCI within 24 h after injury and within 7 days after injury.
This was a retrospective cohort study using Japan Trauma Data Bank (JTDB) which is a nationwide, multicenter database. We selected adult isolated cervical SCI patients who underwent operative management within 7 days after injury, between 2004 and 2015. The main outcome measures were the length of ICU stay and in-hospital mortality. We grouped the patients into two, based on the time from onset of injury to surgery, an early group (within 24 h) and a late group (from 25 h to 7 days). Next, we performed multivariable analyses for analyzing the relevance between the timing of surgery and the length of ICU stay after adjusting for baseline characteristics using propensity score. We also performed the Cox survival analyses to evaluate in-hospital mortality.
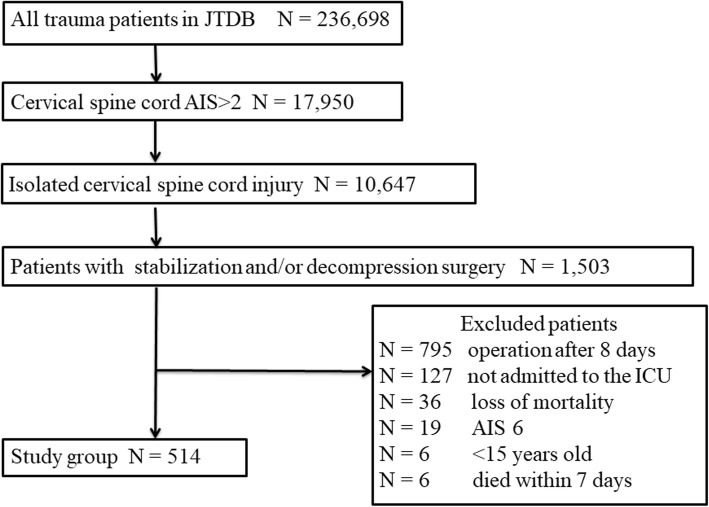
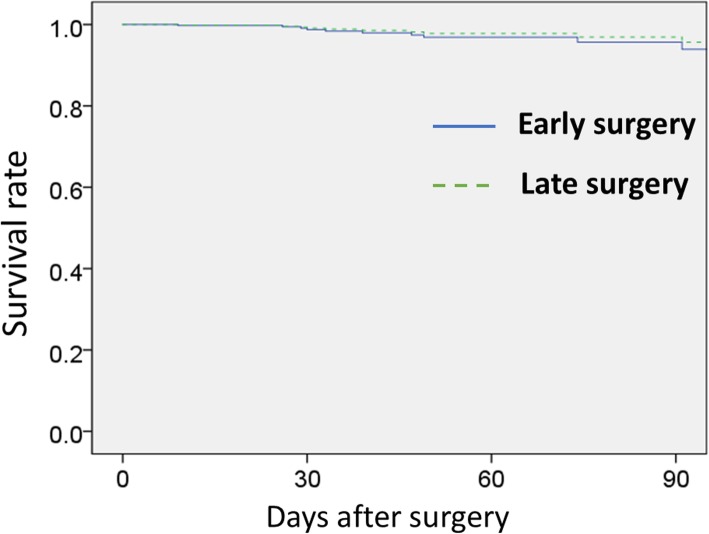
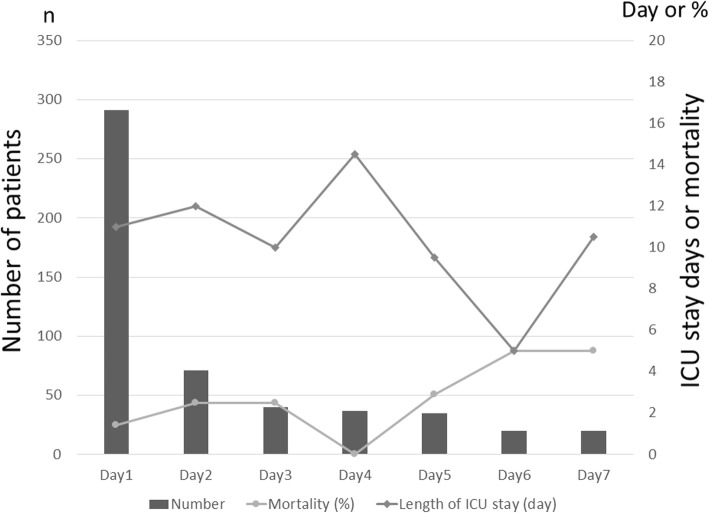
From 236,698 trauma patients registered in JTDB, we analyzed 514 patients. The early group comprised 291 patients (56.6%), and the late group comprised 223 (43.4%). The length of ICU stay did not differ between the two groups (early, 10 days; late, 11 days; p = 0.29). There was no significant difference for length of ICU stay between the early and late group even after adjustment by multivariate analysis (p = 0.64). There was no significant difference in in-hospital mortality between the two groups (the early group 3.8%, the late group 2.2%, p = 0.32), and no significant difference was found in the Cox survival analysis.
Our study showed that neither the length of ICU stay nor in-hospital mortality after spinal column stabilization or spinal cord decompression for cervical SCI significantly differed according to the timing of surgery between 24 h and 7 days.
在过去几十年中,颈椎脊髓损伤(SCI)的治疗方法发生了巨大变化,手术是主要治疗方法。然而,早期手术治疗的最佳时机(伤后 24 小时或 72 小时内)仍存在争议。我们旨在通过比较伤后 24 小时内和伤后 7 天内接受颈椎 SCI 手术(减压和稳定)的患者的 ICU 住院时间和院内死亡率,来确定颈椎 SCI 手术的最佳时机。
这是一项使用日本创伤数据库(JTDB)进行的回顾性队列研究,该数据库是一个全国性的多中心数据库。我们选择了 2004 年至 2015 年间在伤后 7 天内接受手术治疗的成年单纯性颈椎 SCI 患者。主要观察指标是 ICU 住院时间和院内死亡率。我们根据从发病到手术的时间将患者分为两组,即早期组(24 小时内)和晚期组(25 小时至 7 天)。接下来,我们通过倾向评分对基本特征进行调整后,进行多变量分析,以分析手术时机与 ICU 住院时间之间的相关性。我们还进行了 Cox 生存分析,以评估院内死亡率。
从 JTDB 登记的 236698 名创伤患者中,我们分析了 514 名患者。早期组包括 291 名患者(56.6%),晚期组包括 223 名患者(43.4%)。两组 ICU 住院时间无差异(早期 10 天;晚期 11 天;p=0.29)。即使在多变量分析调整后,两组 ICU 住院时间也没有差异(p=0.64)。两组院内死亡率无差异(早期组 3.8%,晚期组 2.2%;p=0.32),Cox 生存分析也无差异。
我们的研究表明,颈椎 SCI 脊柱固定或脊髓减压后 ICU 住院时间和院内死亡率均与 24 小时至 7 天内手术时机无显著差异。