Deakin University, Faculty of Health, Institute for Health Transformation, Deakin Health Economics, Geelong, Victoria, Australia
Deakin University, Faculty of Health, Institute for Health Transformation, Deakin Health Economics, Geelong, Victoria, Australia.
BMJ Open. 2019 Sep 5;9(9):e031033. doi: 10.1136/bmjopen-2019-031033.
Assessing the cost-effectiveness credentials of this intervention in patients with concomitant atrial fibrillation (AF) and heart failure (HF) compared with usual medical therapy.
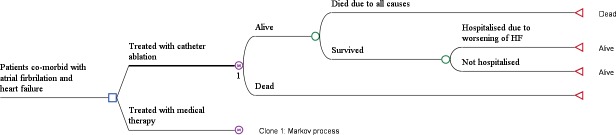
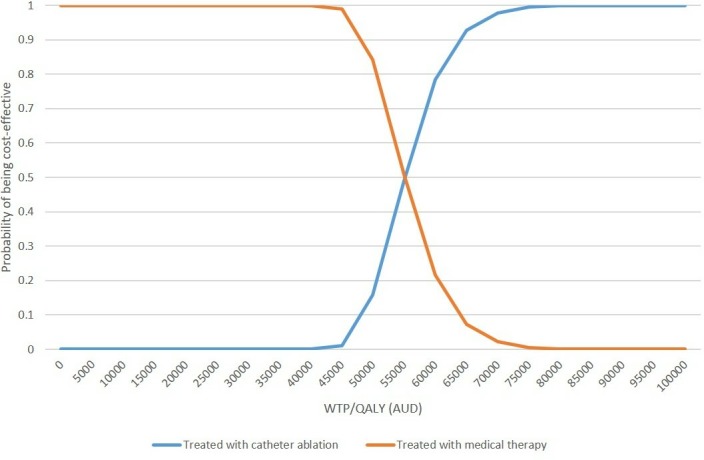
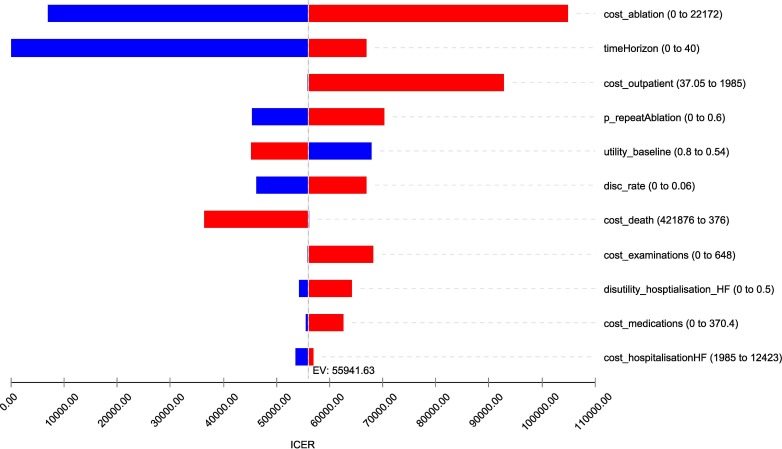
A Markov model comprising two health states (ie, alive or dead) was constructed. The transition probabilities were directly derived from published Kaplan-Meier curves of the pivotal randomised controlled trial and extrapolated over the cohort's lifetime using recommended methods. Costs of catheter ablation, outpatient consultations, hospitalisation, medications and examinations were included. Resource use and unit costs were sourced from government websites or published literature. A lifetime horizon and a healthcare system perspective were taken. All costs and benefits were discounted at 3% annually. Deterministic (DSA) and probabilistic sensitivity analyses (PSA) were run around the key model parameters to test the robustness of the base case results.
A hypothetical Australian cohort of patients with concomitant AF and HF who are resistant to antiarrhythmic treatment.
Catheter ablation versus medical therapy.
The catheter ablation was associated with a cost of $A44 377 per person, in comparison to $A28 506 for the medical therapy alone over a lifetime. Catheter ablation contributed to 4.58 quality-adjusted life years (QALYs) and 6.99 LY gains compared with 4.30 QALYs and 6.53 LY gains, respectively, in the medical therapy arm. The incremental cost-effectiveness ratio was $A55 942/QALY or $A35 020/LY. The DSA showed that results were highly sensitive to costs of ablation and time horizon. The PSA yielded very consistent results with the base case.
Offering catheter ablation procedure to patients with systematic paroxysmal or persistent AF who failed to respond to antiarrhythmic drugs was associated with higher costs, greater benefits. When compared with medical therapy alone, this intervention is not cost-effective from an Australia healthcare system perspective.
评估与常规药物治疗相比,该干预措施在伴有心房颤动(AF)和心力衰竭(HF)的患者中的成本效益。
构建了一个包含两个健康状态(即生存或死亡)的马尔可夫模型。转移概率直接来自关键随机对照试验的已发表的 Kaplan-Meier 曲线,并使用推荐的方法对队列的整个生命周期进行了外推。导管消融、门诊咨询、住院、药物和检查费用均包括在内。资源使用和单位成本来源于政府网站或已发表的文献。采用终生和医疗保健系统视角。所有成本和收益均按每年 3%贴现。针对关键模型参数进行确定性分析(DSA)和概率敏感性分析(PSA),以检验基础案例结果的稳健性。
对心律失常治疗有抵抗作用的伴有 AF 和 HF 的澳大利亚假设队列患者。
导管消融与药物治疗。
在终生范围内,与单独药物治疗相比,导管消融的费用为每人 44377 澳元,而单独药物治疗的费用为 28506 澳元。与药物治疗组相比,导管消融可获得 4.58 个质量调整生命年(QALY)和 6.99 个生命年获益,而药物治疗组分别获得 4.30 个 QALY 和 6.53 个生命年获益。增量成本效益比为 55942 澳元/QALY 或 35020 澳元/LY。DSA 表明结果对消融成本和时间范围高度敏感。PSA 与基础案例产生了非常一致的结果。
对于接受抗心律失常药物治疗后仍未缓解的持续性或阵发性系统性 AF 患者,提供导管消融术可能会带来更高的成本和更大的收益。从澳大利亚医疗保健系统的角度来看,与单独药物治疗相比,该干预措施并不具有成本效益。