Huang Xiyi, Yang Shaomin, Chen Xinjie, Zhao Qiang, Pan Jialing, Lai Shaofen, Ouyang Fusheng, Deng Lingda, Du Yongxing, Chen Jiacheng, Hu Qiugen, Guo Baoliang, Liu Jiemei
Department of Clinical Laboratory, The Affiliated Shunde Hospital of Guangzhou Medical University, Foshan, China.
Department of Radiology, The Affiliated Shunde Hospital of Guangzhou Medical University, Foshan, China.
Front Cardiovasc Med. 2022 Oct 4;9:976844. doi: 10.3389/fcvm.2022.976844. eCollection 2022.
The risk factors for acute heart failure (AHF) vary, reducing the accuracy and convenience of AHF prediction. The most common causes of AHF are coronary heart disease (CHD). A short-term clinical predictive model is needed to predict the outcome of AHF, which can help guide early therapeutic intervention. This study aimed to develop a clinical predictive model for 1-year prognosis in CHD patients combined with AHF.
A retrospective analysis was performed on data of 692 patients CHD combined with AHF admitted between January 2020 and December 2020 at a single center. After systemic treatment, patients were discharged and followed up for 1-year for major adverse cardiovascular events (MACE). The clinical characteristics of all patients were collected. Patients were randomly divided into the training ( = 484) and validation cohort ( = 208). Step-wise regression using the Akaike information criterion was performed to select predictors associated with 1-year MACE prognosis. A clinical predictive model was constructed based on the selected predictors. The predictive performance and discriminative ability of the predictive model were determined using the area under the curve, calibration curve, and clinical usefulness.
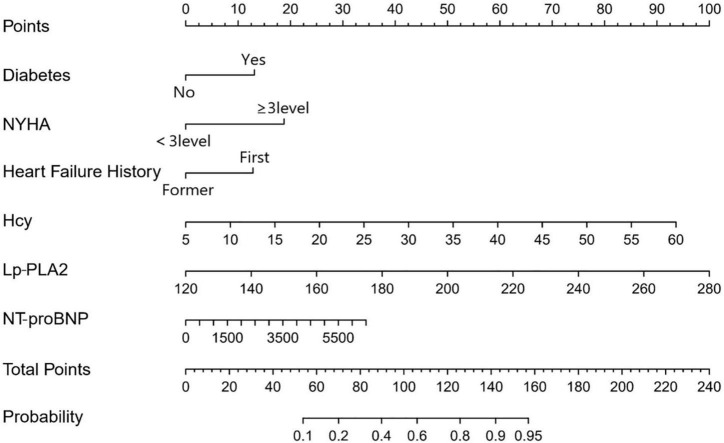
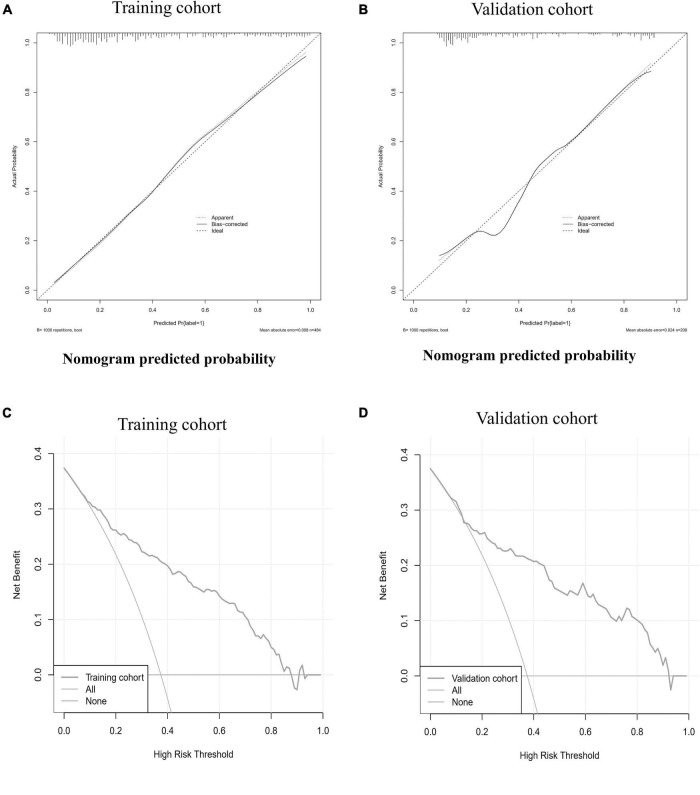
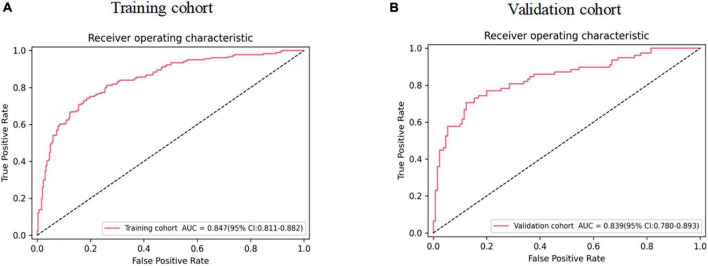
On step-wise regression analysis of the training cohort, predictors for MACE of CHD patients combined with AHF were diabetes, NYHA ≥ 3, HF history, Hcy, Lp-PLA2, and NT-proBNP, which were incorporated into the predictive model. The AUC of the predictive model was 0.847 [95% confidence interval (CI): 0.811-0.882] in the training cohort and 0.839 (95% CI: 0.780-0.893) in the validation cohort. The calibration curve indicated good agreement between prediction by nomogram and actual observation. Decision curve analysis showed that the nomogram was clinically useful.
The proposed clinical prediction model we have established is effective, which can accurately predict the occurrence of early MACE in CHD patients combined with AHF.
急性心力衰竭(AHF)的危险因素各不相同,这降低了AHF预测的准确性和便利性。AHF最常见的病因是冠心病(CHD)。需要一种短期临床预测模型来预测AHF的预后,这有助于指导早期治疗干预。本研究旨在建立一种针对合并AHF的CHD患者1年预后的临床预测模型。
对2020年1月至2020年12月在某单一中心收治的692例合并AHF的CHD患者的数据进行回顾性分析。经过系统治疗后,患者出院并随访1年,观察主要不良心血管事件(MACE)。收集所有患者的临床特征。患者被随机分为训练队列(n = 484)和验证队列(n = 208)。使用赤池信息准则进行逐步回归,以选择与1年MACE预后相关的预测因素。基于所选预测因素构建临床预测模型。使用曲线下面积、校准曲线和临床实用性来确定预测模型的预测性能和判别能力。
在训练队列的逐步回归分析中,合并AHF的CHD患者MACE的预测因素为糖尿病、纽约心脏协会(NYHA)心功能分级≥3级、心力衰竭病史、同型半胱氨酸(Hcy)、脂蛋白相关磷脂酶A2(Lp-PLA2)和N末端脑钠肽前体(NT-proBNP),这些因素被纳入预测模型。预测模型在训练队列中的曲线下面积(AUC)为0.847 [95%置信区间(CI):0.811 - 0.882],在验证队列中为0.839(95%CI:0.780 - 0.893)。校准曲线表明列线图预测与实际观察之间具有良好的一致性。决策曲线分析表明列线图具有临床实用性。
我们建立的临床预测模型是有效的,能够准确预测合并AHF的CHD患者早期MACE的发生。