Musculoskeletal Research Unit, Translational Health Sciences, Bristol Medical School, University of Bristol, Bristol, UK
Musculoskeletal Research Unit, Translational Health Sciences, Bristol Medical School, University of Bristol, Bristol, UK.
BMJ Open. 2019 Sep 6;9(9):e028093. doi: 10.1136/bmjopen-2018-028093.
For many people with advanced osteoarthritis, total knee replacement (TKR) is an effective treatment for relieving pain and improving function. Features of perioperative care may be associated with the adverse event of chronic pain 6 months or longer after surgery; effects may be direct, for example, through nerve damage or surgical complications, or indirect through adverse events. This systematic review aims to evaluate whether non-surgical perioperative interventions prevent long-term pain after TKR.
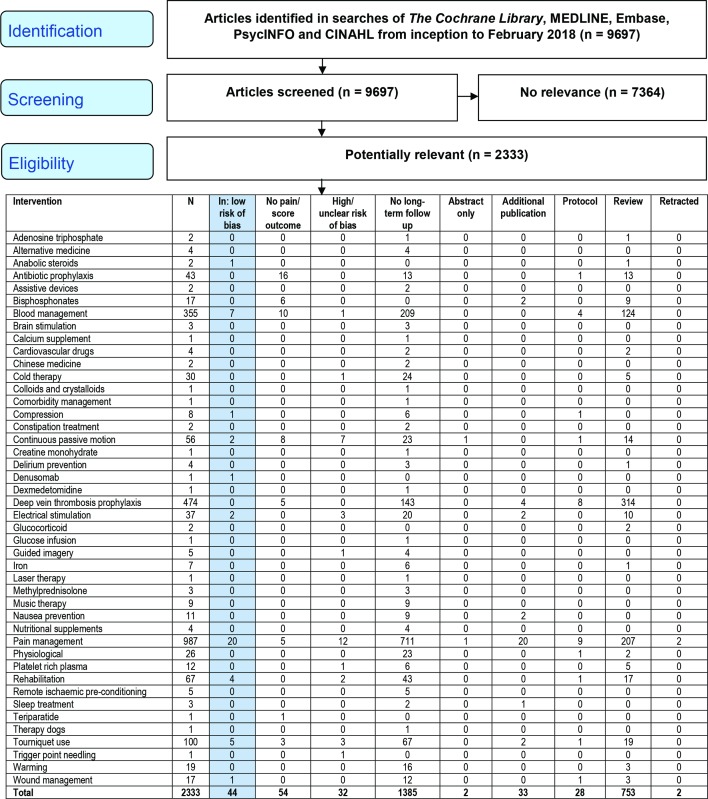
We conducted a systematic review of perioperative interventions for adults with osteoarthritis receiving primary TKR evaluated in a randomised controlled trial (RCT). We searched , MEDLINE, Embase, PsycINFO and CINAHL until February 2018. After screening, two reviewers evaluated articles. Studies at low risk of bias according to the Cochrane tool were included.
Perioperative non-surgical interventions; control receiving no intervention or alternative treatment.
Pain or score with pain component assessed at 6 months or longer postoperative.
44 RCTs at low risk of bias assessed long-term pain. Intervention heterogeneity precluded meta-analysis and definitive statements on effectiveness. Good-quality research provided generally weak evidence for small reductions in long-term pain with local infiltration analgesia (three studies), ketamine infusion (one study), pregabalin (one study) and supported early discharge (one study) compared with no intervention. For electric muscle stimulation (two studies), anabolic steroids (one study) and walking training (one study) there was a suggestion of more clinically important benefit. No concerns relating to long-term adverse events were reported. For a range of treatments there was no evidence linking them with unfavourable pain outcomes.
To prevent chronic pain after TKR, several perioperative interventions show benefits and merit further research. Good-quality studies assessing long-term pain after perioperative interventions are feasible and necessary to ensure that patients with osteoarthritis achieve good long-term outcomes after TKR.
对于许多患有晚期骨关节炎的人来说,全膝关节置换术(TKR)是一种有效缓解疼痛和改善功能的治疗方法。围手术期护理的特点可能与术后 6 个月或更长时间的慢性疼痛不良事件有关;这些影响可能是直接的,例如通过神经损伤或手术并发症,也可能是间接的,例如通过不良事件。本系统评价旨在评估围手术期非手术干预措施是否能预防 TKR 后长期疼痛。
我们对接受初次 TKR 的骨关节炎成人进行了围手术期干预的系统评价,这些研究采用了随机对照试验(RCT)。我们检索了、MEDLINE、Embase、PsycINFO 和 CINAHL,直到 2018 年 2 月。经过筛选,两名审查员评估了文章。根据 Cochrane 工具评估为低偏倚风险的研究被纳入。
围手术期非手术干预;对照组接受无干预或替代治疗。
术后 6 个月或更长时间评估疼痛或疼痛成分评分。
44 项低偏倚风险 RCT 评估了长期疼痛。干预措施的异质性排除了荟萃分析和有效性的明确结论。高质量的研究为局部浸润性镇痛(三项研究)、氯胺酮输注(一项研究)、普瑞巴林(一项研究)和支持早期出院(一项研究)与无干预相比,长期疼痛有较小的降低提供了一般较弱的证据。对于电肌肉刺激(两项研究)、合成代谢类固醇(一项研究)和步行训练(一项研究),有更多的临床重要益处的提示。没有报告与长期不良事件有关的问题。对于一系列治疗方法,没有证据表明它们与不利的疼痛结果有关。
为了预防 TKR 后慢性疼痛,一些围手术期干预措施显示出益处,值得进一步研究。评估围手术期干预后长期疼痛的高质量研究是可行的,也是必要的,以确保骨关节炎患者在 TKR 后获得良好的长期结果。