Usman Atif, Makmor Bakry Mohd, Mustafa Norlaila, Rehman Inayat Ur, Bukhsh Allah, Lee Shaun Wen Huey, Khan Tahir Mehmood
School of Pharmacy, Monash University, Bandar Sunway, Selangor, Malaysia.
Faculty of Pharmacy, Universiti Kebangsaan Malaysia, Kuala Lumpur, Malaysia.
Diabetes Metab Syndr Obes. 2019 Aug 6;12:1323-1338. doi: 10.2147/DMSO.S208492. eCollection 2019.
During the progress and resolution of a diabetic ketoacidosis (DKA) episode, potassium levels are significantly affected by the extent of acidosis. However, none of the current guidelines take into account acidosis during resuscitation of potassium level in DKA management, which may increase the risk of cardiovascular adverse events.
To assess literature regarding the adjustment of potassium level using pH to calculate pH-adjusted corrected potassium level, and to observe the relationship of cardiovascular outcomes with reported potassium level and pH-adjusted corrected potassium in DKA.
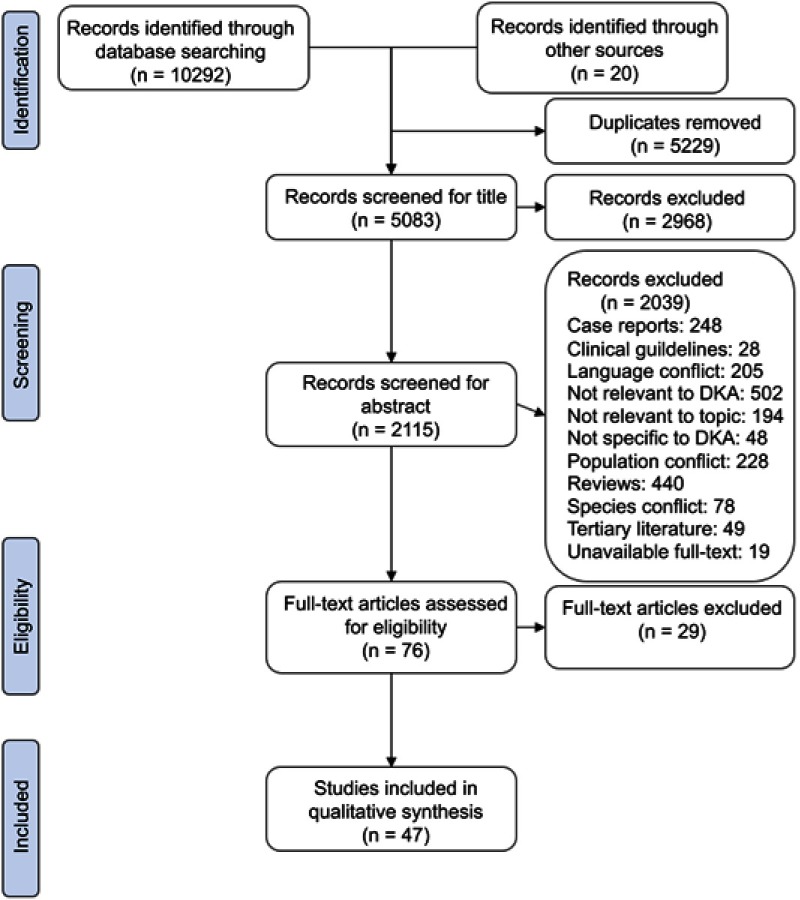
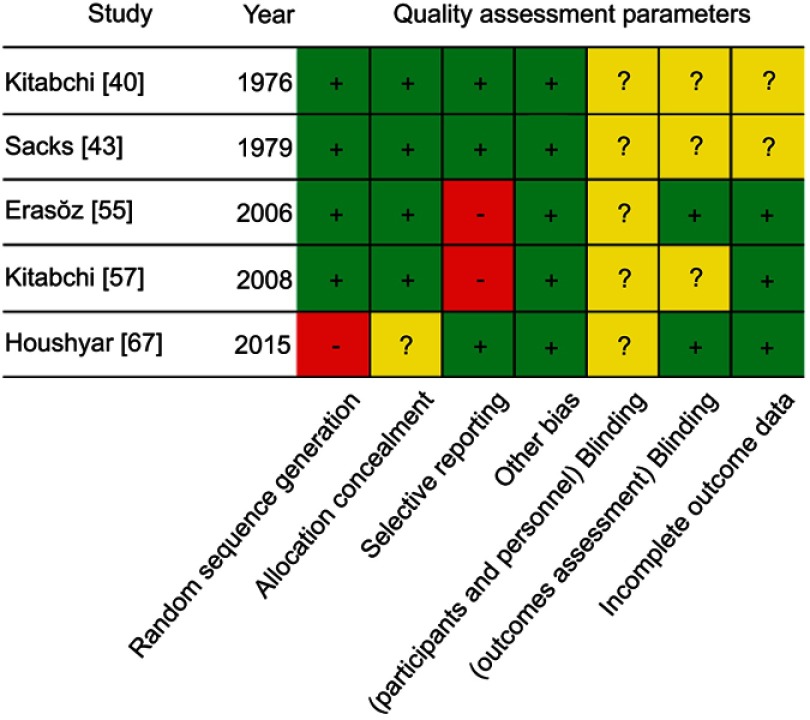
Seven databases were searched from inception to January 2018 for studies which had reported people with diabetes developing diabetic ketoacidosis, in relation to prevalence or incidence, fluid resuscitation or potassium supplementation treatment, treatment or cardiovascular outcomes, and experimentation with DKA management or insulin. Quality of studies was evaluated using Cochrane Risk of Bias and Newcastle Ottawa Scale.
Forty-seven studies were included in qualitative synthesis out of a total of 10,292 retrieved studies. Forty-one studies discussed the potassium level and blood pH at the time of admission, ten studies discussed cardiovascular outcomes, and only four studies concurrently discussed potassium level, pH, and cardiovascular outcomes. Only two studies were graded as good on the Newcastle Ottawa Scale. The reported potassium level was well within normal range (5.8 mmol/L), whereas pH rendered patients to be moderately acidotic (7.13). Surprisingly, none of the included studies mentioned pH-adjusted corrected potassium level and, hence, this was calculated later. Although mean corrected potassium was within the normal range (3.56 mmol/L), 13 studies had corrected potassium below 3.5 mmol/L and five had it below 3.0 mmol/L. Nevertheless, with the exception of one study, none discussed cardiovascular outcomes in the context of potassium or pH-adjusted potassium level.
The evidence surrounding cardiovascular outcomes during DKA episodes in light of a pH-adjusted corrected potassium level is scarce. A prospective observational, or preferably, an experimental study in this regard will ensure we can modify and enhance safety of existing DKA treatment protocols.
在糖尿病酮症酸中毒(DKA)发作的进展和缓解过程中,血钾水平受酸中毒程度的显著影响。然而,当前所有指南在DKA管理中纠正血钾水平的复苏过程中均未考虑酸中毒情况,这可能会增加心血管不良事件的风险。
评估关于使用pH值计算pH校正后血钾水平以调整血钾水平的文献,并观察DKA中报告的血钾水平和pH校正后血钾与心血管结局之间的关系。
检索了7个数据库,从建库至2018年1月,查找报告糖尿病患者发生糖尿病酮症酸中毒的研究,内容涉及患病率或发病率、液体复苏或补钾治疗、治疗或心血管结局以及DKA管理或胰岛素实验。使用Cochrane偏倚风险评估和纽卡斯尔渥太华量表评估研究质量。
在总共检索到的10292项研究中,有47项研究纳入了定性综合分析。41项研究讨论了入院时的血钾水平和血pH值,10项研究讨论了心血管结局,只有4项研究同时讨论了血钾水平、pH值和心血管结局。在纽卡斯尔渥太华量表上,只有2项研究被评为高质量。报告的血钾水平在正常范围内(5.8 mmol/L),而pH值使患者处于中度酸中毒状态(7.13)。令人惊讶的是,纳入的研究均未提及pH校正后血钾水平,因此,随后进行了计算。尽管校正后血钾的平均值在正常范围内(3.56 mmol/L),但有13项研究的校正后血钾低于3.5 mmol/L,5项研究低于3.0 mmol/L。然而,除一项研究外,没有研究在血钾或pH校正后血钾水平的背景下讨论心血管结局。
鉴于pH校正后血钾水平,关于DKA发作期间心血管结局的证据很少。在这方面进行前瞻性观察研究,或者最好是实验性研究,将确保我们能够修改和提高现有DKA治疗方案的安全性。