Bouksila Mouna, Mrad Mehdi, Kaabachi Wajih, Kalai Eya, Smaoui Wided, Rekik Sonia, Krir Asma, Issaoui Nesrine, Hamzaoui Kamel, Sahli Hela, Kateb Elhem Cheour El, Zouaghi Mohammed Karim, Bahlous Afef
Immuno-Rheumatology Research Laboratory, Rheumatology Department, La Rabta Hospital, University of Tunis-El Manar, Tunis, Tunisia.
Laboratory of Clinical Biochemistry and Hormonology; Pasteur Institute of Tunis, University of Tunis-El Manar, Tunis, Tunisia.
J Med Biochem. 2019 Jul 30;38(4):418-426. doi: 10.2478/jomb-2019-0002. eCollection 2019 Oct.
Chronic kidney disease (CKD) is associated with numerous complications such as bone mineral disorder. The aim of our study was to analyze the correlation of bone turnover markers with Bone Mineral Density (BMD) measurements in Tunisian end stage renal diseases (ESRD) patients.
This study included 100 ESRD Tunisian patients. Their estimated glomerular filtration rate (eGFR) was < 15 mL × min × (1.73 m), which requires hemodialysis. Bone-specific alkaline phosphatase (BALP) serum concentration was determined with a chemiluminescence immunoassay. Fibroblast Growth Factor 23 (FGF23) serum was assessed by Enzyme-Linked Immunosorbent Assay method. The serum levels of 25-Hydroxyvitamin D (25(OH)D), intact parathyroid hormone (iPTH) and Beta cross-laps (CTX) was measured by Electrochemiluminescence Technology. DEXA (dual-energy x-ray absorptiometry) technique was used to evaluate BMD.
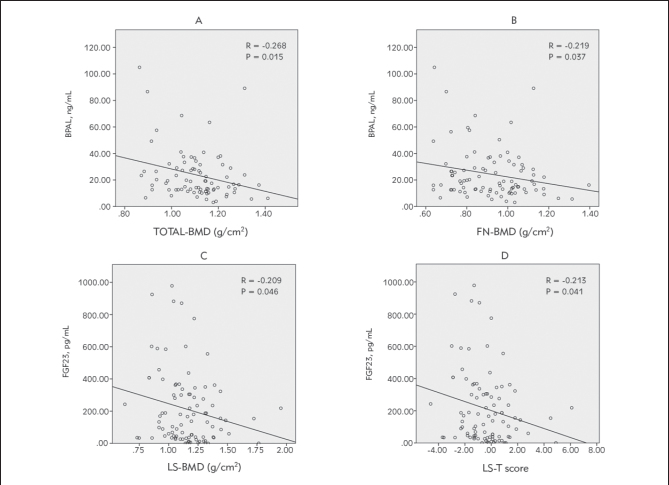
We observed a statistically significant negative correlation between BALP levels and total body BMD (r = -0.268; P = 0.015) particularly in femoral neck (FN) (r = -0.219; P = 0.037). BALP concentrations were negatively associated with total BMD especially in FN for patients with BMI < 30, FGF23 concentrations were also negatively correlated with BMD in lumbar spine site (LS) (r = -0.209; P = 0.046). For osteopenic patients we found an inverse correlation between 25(OH)D concentrations and BMD in LS position (r = -0.336; P = 0.038). In men group, we have also found a negative correlation between iPTH and total BMD (r = -0.326; P = 0.015). However we found a positive correlation between calcium expression and BMD in LS site (r = 0.270; P = 0.031).
FGF23 and BALP can predict bone loss in ESRD through their strong correlation with BMD in LS and FN sites respectively.
慢性肾脏病(CKD)与诸多并发症相关,如骨矿物质紊乱。我们研究的目的是分析突尼斯终末期肾病(ESRD)患者骨转换标志物与骨密度(BMD)测量值之间的相关性。
本研究纳入了100名突尼斯ESRD患者。他们的估算肾小球滤过率(eGFR)<15 mL×min×(1.73 m²),需要进行血液透析。采用化学发光免疫分析法测定血清骨特异性碱性磷酸酶(BALP)浓度。通过酶联免疫吸附测定法评估血清成纤维细胞生长因子23(FGF23)。采用电化学发光技术测量血清25-羟维生素D(25(OH)D)、完整甲状旁腺激素(iPTH)和β-交联羧基端肽(CTX)水平。使用双能X线吸收法(DEXA)技术评估骨密度。
我们观察到BALP水平与全身骨密度之间存在统计学显著负相关(r = -0.268;P = 0.015),特别是在股骨颈(FN)部位(r = -0.219;P = 0.037)。对于体重指数(BMI)<30的患者,BALP浓度与全身骨密度呈负相关,尤其是在FN部位;FGF23浓度与腰椎(LS)部位的骨密度也呈负相关(r = -0.209;P = 0.046)。对于骨质减少患者,我们发现25(OH)D浓度与LS部位的骨密度呈负相关(r = -0.336;P = 0.038)。在男性组中,我们还发现iPTH与全身骨密度呈负相关(r = -0.326;P = 0.015)。然而,我们发现钙表达与LS部位的骨密度呈正相关(r = 0.270;P = 0.031)。
FGF23和BALP分别通过与LS和FN部位的骨密度密切相关,可预测ESRD患者的骨质流失。