Division of Clinical Pharmacology, Department of Medicine, Vanderbilt University Medical Center, Nashville, Tennessee.
Department of Biomedical Informatics, Vanderbilt University Medical Center, Nashville, Tennessee.
JAMA Netw Open. 2019 Sep 4;2(9):e1911130. doi: 10.1001/jamanetworkopen.2019.11130.
Whether the PCSK9 gene is associated with the progress from infection to sepsis is unknown to date.
To test the associations between PCSK9 genetic variants, a PCSK9 genetic risk score (GRS), or genetically estimated PCSK9 expression levels and the risk of sepsis among patients admitted to a hospital with infection.
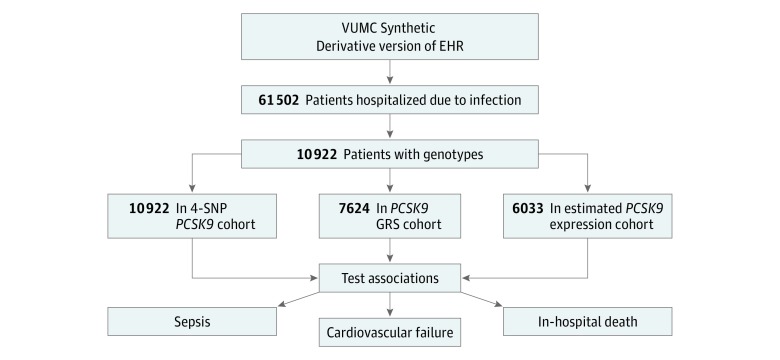
DESIGN, SETTING, AND PARTICIPANTS: This retrospective cohort study used deidentified electronic health records to identify patients admitted to Vanderbilt University Medical Center, Nashville, Tennessee, with infection. Patients were white adults, had a code indicating infection from the International Classification of Diseases, Ninth Revision, Clinical Modification, or the International Statistical Classification of Diseases, Tenth Revision, Clinical Modification, and received an antibiotic within 1 day of hospital admission (N = 61 502). Data were collected from January 1, 1993, through December 31, 2017, and analyzed from April 1, 2018, to March 16, 2019.
Four known PCSK9 functional variants, a GRS for PCSK9, and genetically estimated PCSK9 expression.
The primary outcome was sepsis; secondary outcomes included cardiovascular failure and in-hospital death.
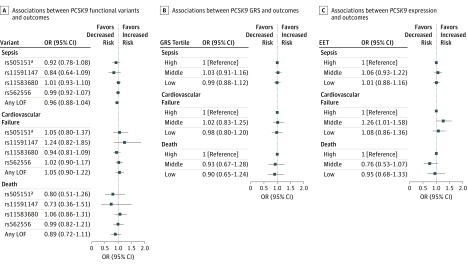
Of patients with infection, genotype information was available in 10 922 white patients for PCSK9 functional variants (5628 men [51.5%]; mean [SD] age, 60.1 [15.7] years), including 7624 patients with PCSK9 GRS and 6033 patients with estimated PCSK9 expression. Of these, 3391 developed sepsis, 835 developed cardiovascular failure, and 366 died during hospitalization. None of the 4 functional PCSK9 variants were significantly associated with sepsis, cardiovascular failure, or in-hospital death, with or without adjustment for (1) age and sex or (2) age, sex, and Charlson-Deyo comorbidities (in model adjusted for age, sex, and comorbidities, odds ratios for any loss-of function variant were 0.96 [95% CI, 0.88-1.04] for sepsis, 1.05 [95% CI, 0.90-1.22] for cardiovascular failure, and 0.89 [95% CI, 0.72-1.11] for death). Similarly, neither the PCSK9 GRS nor genetically estimated PCSK9 expression were significantly associated with sepsis, cardiovascular failure, or in-hospital death in any of the analysis models. For GRS, in the full model adjusted for age, sex, and comorbidities, the odds ratios were 1.01 for sepsis (95% CI, 0.96-1.06; P = .70), 1.03 for cardiovascular failure (95% CI, 0.95-1.12; P = .48), and 1.05 for in-hospital death (95% CI, 0.92-1.19; P = .50). For genetically estimated PCSK9 expression, in the full model adjusted for age, sex, and comorbidities, the odds ratios were 1.01 for sepsis (95% CI, 0.95-1.06; P = .86), 0.96 for cardiovascular failure (95% CI, 0.88-1.05; P = .41), and 0.99 for in-hospital death (95% CI, 0.87-1.14; P = .94).
In this study, PCSK9 genetic variants were not significantly associated with risk of sepsis or the outcomes of sepsis in patients hospitalized with infection.
重要性:目前尚不清楚载脂蛋白 B 分泌酶 9(PCSK9)基因是否与从感染进展为败血症有关。
目的:检测 PCSK9 遗传变异、PCSK9 遗传风险评分(GRS)或遗传估计的 PCSK9 表达水平与感染住院患者败血症风险之间的关系。
设计、设置和参与者:这项回顾性队列研究使用去识别的电子健康记录来确定田纳西州纳什维尔范德比尔特大学医学中心因感染而住院的患者。患者为白人成年人,国际疾病分类,第九修订版,临床修正(International Classification of Diseases, Ninth Revision, Clinical Modification)或国际疾病分类,第十修订版,临床修正(International Statistical Classification of Diseases, Tenth Revision, Clinical Modification)中有编码表示感染,并且在入院后 1 天内接受抗生素治疗(N=61502)。数据收集于 1993 年 1 月 1 日至 2017 年 12 月 31 日,分析时间为 2018 年 4 月 1 日至 2019 年 3 月 16 日。
暴露情况:4 个已知的 PCSK9 功能变异、PCSK9 GRS 和遗传估计的 PCSK9 表达。
主要结果和措施:主要结局是败血症;次要结局包括心血管衰竭和住院期间死亡。
结果:在感染患者中,10922 名白人患者的 PCSK9 功能变异的基因型信息可用(5628 名男性[51.5%];平均[SD]年龄,60.1[15.7]岁),包括 7624 名 PCSK9 GRS 和 6033 名估计的 PCSK9 表达患者。其中,3391 人发生败血症,835 人发生心血管衰竭,366 人住院期间死亡。在调整(1)年龄和性别或(2)年龄、性别和 Charlson-Deyo 合并症后,4 个功能 PCSK9 变异中的任何失活变异与败血症、心血管衰竭或住院期间死亡均无显著相关性,优势比为任何失活变异的 0.96(95%CI,0.88-1.04)败血症,1.05(95%CI,0.90-1.22)心血管衰竭,0.89(95%CI,0.72-1.11)死亡)。同样,PCSK9 GRS 或遗传估计的 PCSK9 表达在任何分析模型中均与败血症、心血管衰竭或住院期间死亡无显著相关性。对于 GRS,在调整年龄、性别和合并症的全模型中,败血症的优势比为 1.01(95%CI,0.96-1.06;P=0.70),心血管衰竭的优势比为 1.03(95%CI,0.95-1.12;P=0.48),住院期间死亡的优势比为 1.05(95%CI,0.92-1.19;P=0.50)。对于遗传估计的 PCSK9 表达,在调整年龄、性别和合并症的全模型中,败血症的优势比为 1.01(95%CI,0.95-1.06;P=0.86),心血管衰竭的优势比为 0.96(95%CI,0.88-1.05;P=0.41),住院期间死亡的优势比为 0.99(95%CI,0.87-1.14;P=0.94)。
结论和相关性:在这项研究中,PCSK9 遗传变异与感染住院患者败血症风险或败血症结局无显著相关性。