Northwestern University Feinberg School of Medicine, Chicago, IL.
Baylor University Medical Center, Dallas, TX.
Hepatology. 2020 May;71(5):1775-1786. doi: 10.1002/hep.30939. Epub 2020 Jan 28.
A high proportion of patients develop chronic kidney disease (CKD) after liver transplantation (LT). We aimed to develop clinical/protein models to predict future glomerular filtration rate (GFR) deterioration in this population.
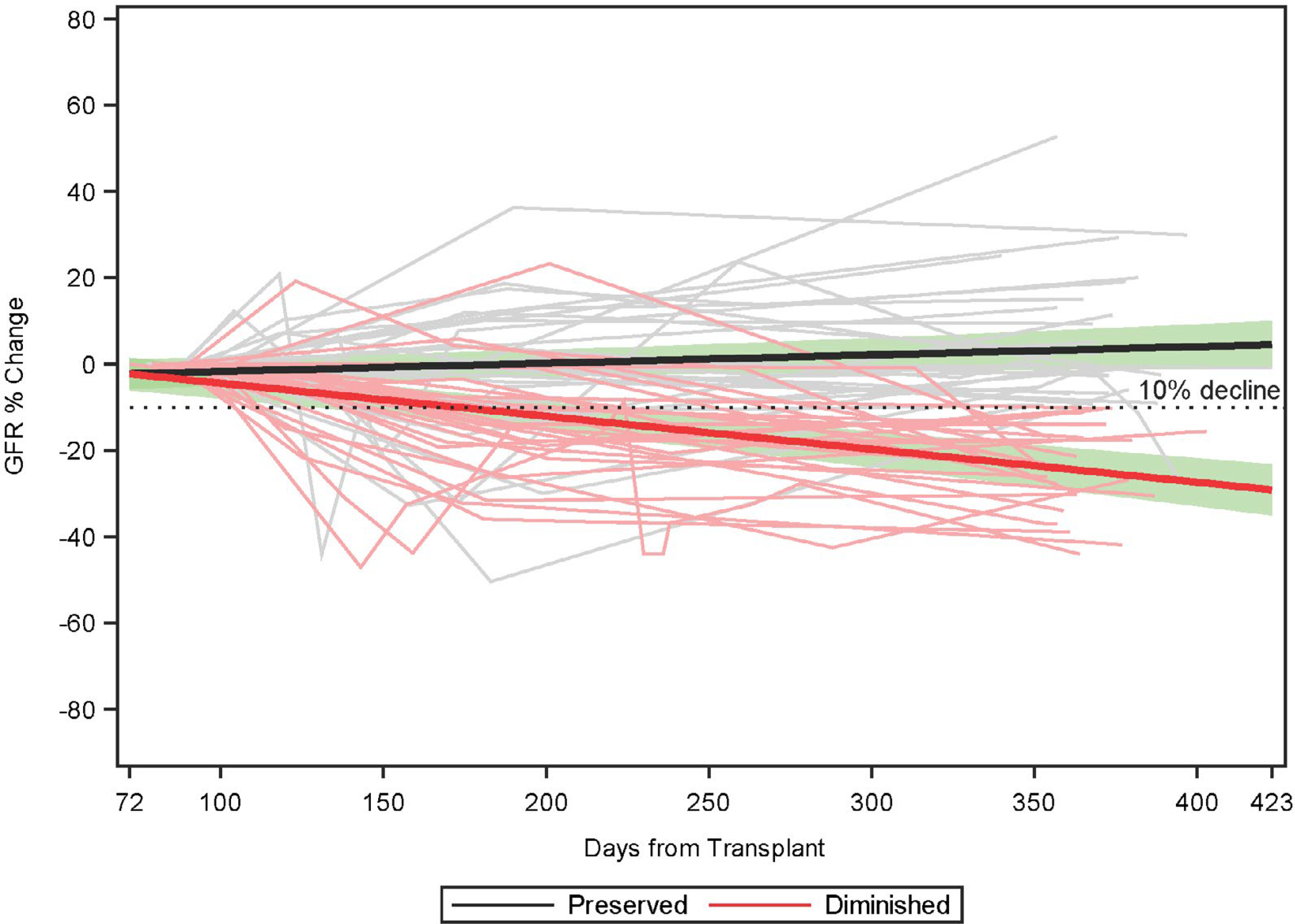
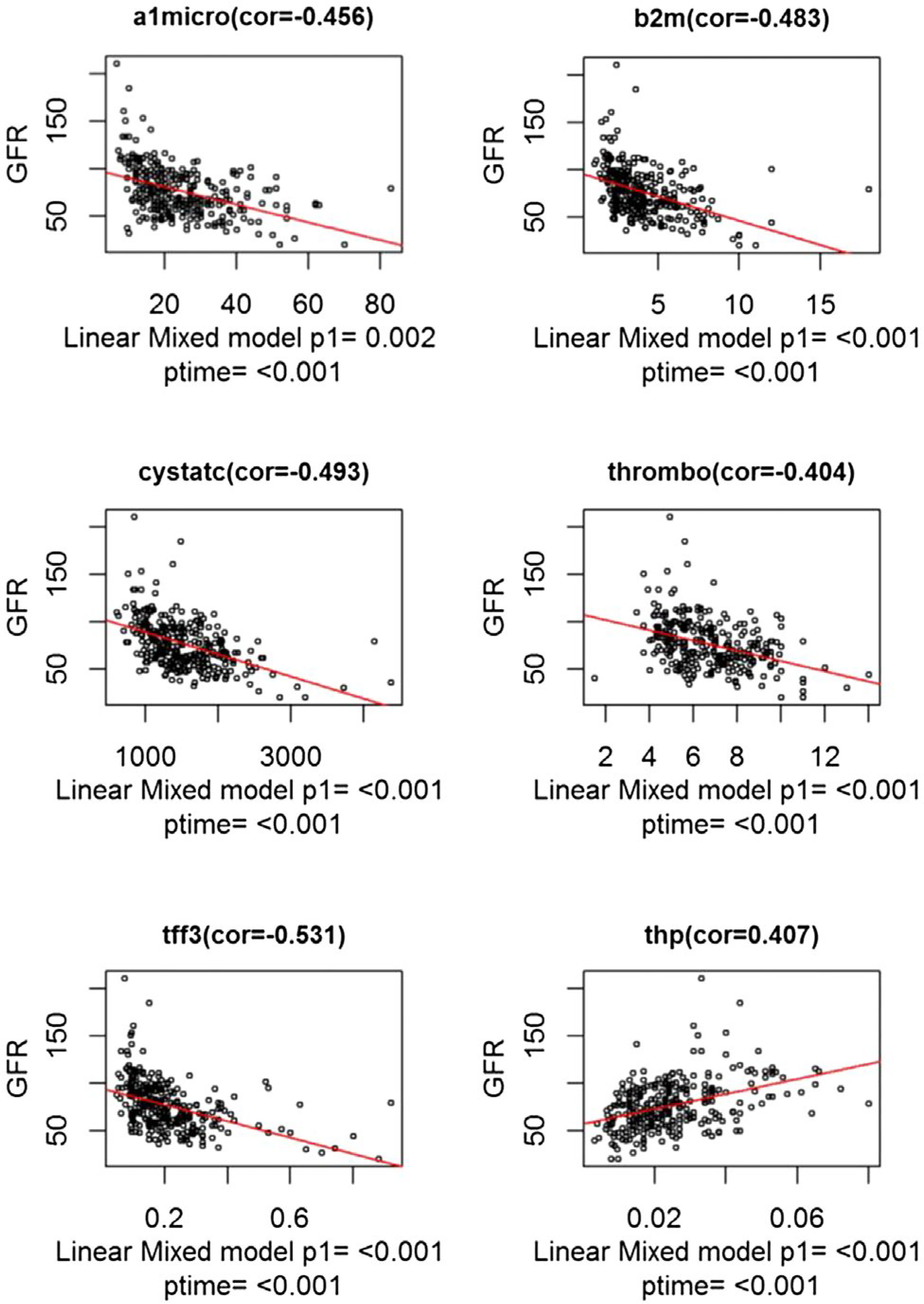
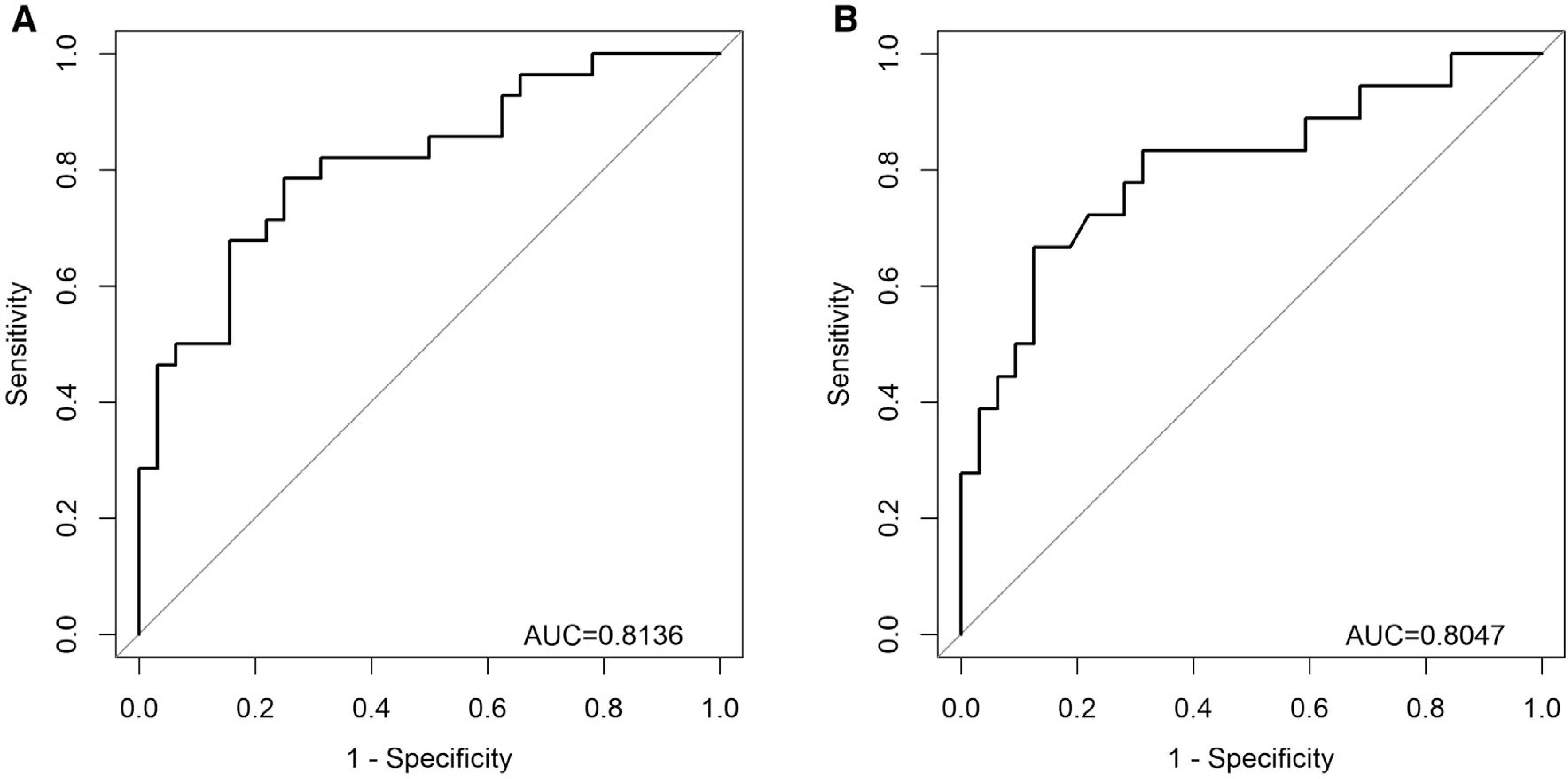
In independent multicenter discovery (CTOT14) and single-center validation (BUMC) cohorts, we analyzed kidney injury proteins in serum/plasma samples at month 3 after LT in recipients with preserved GFR who demonstrated subsequent GFR deterioration versus preservation by year 1 and year 5 in the BUMC cohort. In CTOT14, we also examined correlations between serial protein levels and GFR over the first year. A month 3 predictive model was constructed from clinical and protein level variables using the CTOT14 cohort (n = 60). Levels of β-2 microglobulin and CD40 antigen and presence of hepatitis C virus (HCV) infection predicted early (year 1) GFR deterioration (area under the curve [AUC], 0.814). We observed excellent validation of this model (AUC, 0.801) in the BUMC cohort (n = 50) who had both early and late (year 5) GFR deterioration. At an optimal threshold, the model had the following performance characteristics in CTOT14 and BUMC, respectively: accuracy (0.75, 0.8), sensitivity (0.71, 0.67), specificity (0.78, 0.88), positive predictive value (0.74, 0.75), and negative predictive value (0.76, 0.82). In the serial CTOT14 analysis, several proteins, including β-2 microglobulin and CD40, correlated with GFR changes over the first year.
We have validated a clinical/protein model (PRESERVE) that early after LT can predict future renal deterioration versus preservation with high accuracy. This model may help select recipients at higher risk for subsequent CKD for early, proactive renal sparing strategies.
相当一部分肝移植(LT)术后患者会发展为慢性肾脏病(CKD)。本研究旨在建立临床/蛋白模型,以预测该人群肾小球滤过率(GFR)的未来恶化情况。
在独立的多中心发现(CTOT14)和单中心验证(BUMC)队列中,我们分析了 GFR 保留但在 BUMC 队列中于第 1 年和第 5 年发生 GFR 下降的患者,在 LT 后 3 个月时血清/血浆样本中的肾脏损伤蛋白。在 CTOT14 中,我们还检查了在第 1 年内,连续蛋白水平与 GFR 之间的相关性。使用 CTOT14 队列(n=60),根据临床和蛋白水平变量构建了 3 个月的预测模型。β-2 微球蛋白和 CD40 抗原水平以及丙型肝炎病毒(HCV)感染的存在预测了早期(第 1 年)GFR 恶化(曲线下面积[AUC],0.814)。我们发现该模型在具有早期和晚期(第 5 年)GFR 恶化的 BUMC 队列(n=50)中得到了很好的验证(AUC,0.801)。在最优阈值下,该模型在 CTOT14 和 BUMC 中的表现特征分别为:准确性(0.75,0.8)、灵敏度(0.71,0.67)、特异性(0.78,0.88)、阳性预测值(0.74,0.75)和阴性预测值(0.76,0.82)。在 CTOT14 的连续分析中,包括β-2 微球蛋白和 CD40 在内的几种蛋白与第 1 年内 GFR 的变化相关。
我们验证了一种临床/蛋白模型(PRESERVE),该模型在 LT 后早期可以高准确度预测未来的肾脏恶化与保留情况。该模型可能有助于选择发生后续 CKD 风险较高的受者,以实施早期、积极的肾脏保护策略。