Farley Stephen, Gottesman Malcolm H, Friedman-Urevich Sharon, Ye Janin, Shen Mark, Grueneberg Denise, Martone Lorraine, Calixte Rose
Department of Pharmacy, NYU Winthrop Hospital, Mineola, NY.
NYU Winthrop Hospital, Mineola, NY.
Surg Neurol Int. 2019 Apr 24;10:59. doi: 10.25259/SNI-4-2019. eCollection 2019.
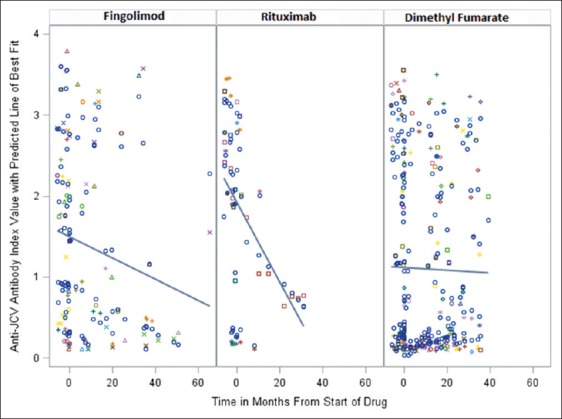
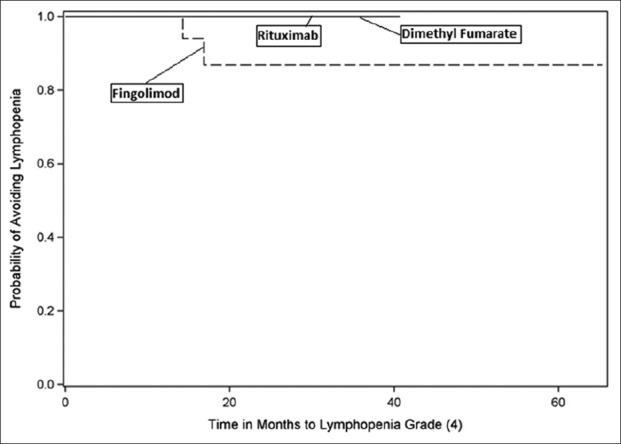
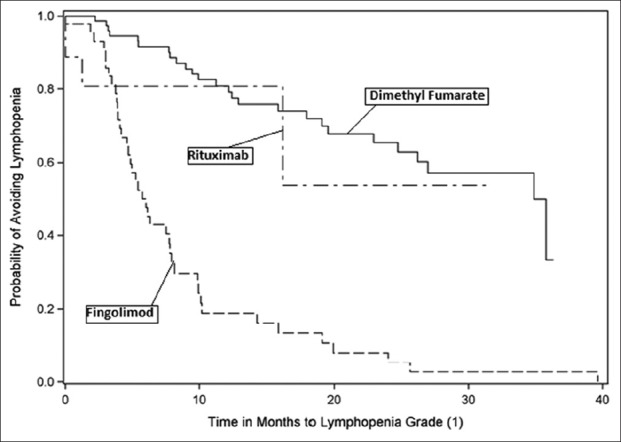
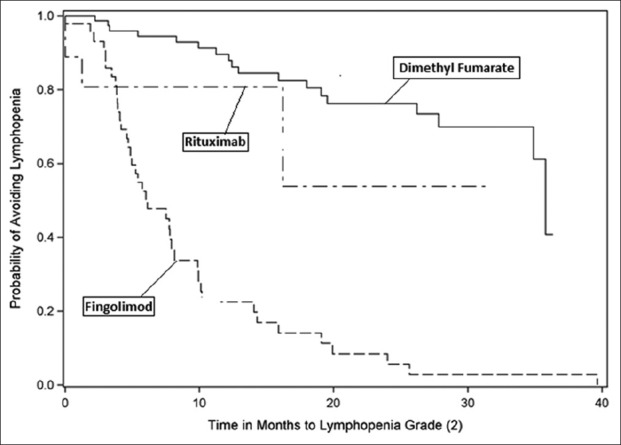
Progressive multifocal leukoencephalopathy (PML), a potentially fatal demyelinating disease caused by the John Cunningham virus (JCV), can occur as a complication of treatment with rituximab, fingolimod, and dimethyl fumarate. The primary objective of this study was to determine changes in anti-JCV antibody index values in multiple sclerosis (MS) patients treated with these three medications. Second, we explored the relationship between absolute lymphocyte count (ALC), anti-JCV antibody index values, and various patient characteristics.
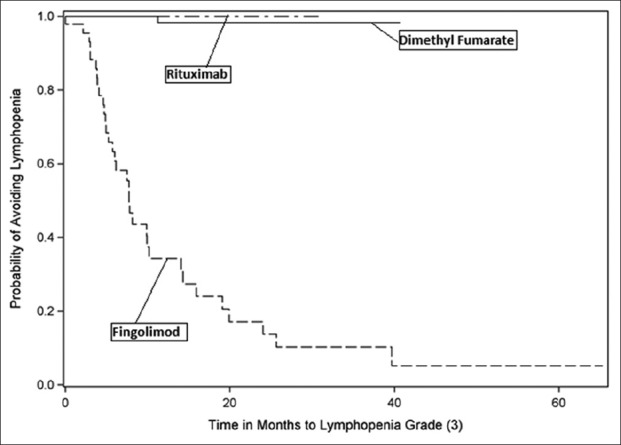
In this retrospective chart review, we evaluated changes in JCV serology and ALC in 172 MS patients treated with fingolimod, rituximab, or dimethyl fumarate (2013-2016). Only those with known anti-JCV antibody and ALC values before starting the study medications were included. Subsequent values were obtained on an ad hoc basis throughout the study.
There was a significant decrease in anti-JCV antibody index values in patients treated with fingolimod and rituximab ( = 0.03 and = 0.014, respectively). A non-significant decreasing trend in anti-JCV antibody index values occurred in patients treated with dimethyl fumarate. Notably, there was no relationship between ALC and anti-JCV antibody index values for patients treated with rituximab, fingolimod, or dimethyl fumarate.
Anti-JCV antibody index values significantly decreased in MS patients treated with fingolimod and rituximab; however, this did not occur with dimethyl fumarate. Fingolimod and rituximab may impair the humoral response to the JCV. Nevertheless, a declining anti-JCV antibody index in MS patients treated with fingolimod or rituximab should not necessarily be interpreted as correlating with a decreased risk for PML.
进行性多灶性白质脑病(PML)是一种由约翰·坎宁安病毒(JCV)引起的潜在致命性脱髓鞘疾病,可作为利妥昔单抗、芬戈莫德和富马酸二甲酯治疗的并发症出现。本研究的主要目的是确定接受这三种药物治疗的多发性硬化症(MS)患者抗JCV抗体指数值的变化。其次,我们探讨了绝对淋巴细胞计数(ALC)、抗JCV抗体指数值与各种患者特征之间的关系。
在这项回顾性病历审查中,我们评估了172例接受芬戈莫德、利妥昔单抗或富马酸二甲酯治疗的MS患者(2013 - 2016年)的JCV血清学和ALC变化。仅纳入在开始研究药物治疗前已知抗JCV抗体和ALC值的患者。在整个研究过程中根据需要获取后续值。
接受芬戈莫德和利妥昔单抗治疗的患者抗JCV抗体指数值显著下降(分别为P = 0.03和P = 0.014)。接受富马酸二甲酯治疗的患者抗JCV抗体指数值出现非显著下降趋势。值得注意的是,接受利妥昔单抗、芬戈莫德或富马酸二甲酯治疗的患者,其ALC与抗JCV抗体指数值之间没有关系。
接受芬戈莫德和利妥昔单抗治疗的MS患者抗JCV抗体指数值显著下降;然而,富马酸二甲酯治疗并未出现这种情况。芬戈莫德和利妥昔单抗可能会损害对JCV的体液免疫反应。尽管如此,接受芬戈莫德或利妥昔单抗治疗的MS患者抗JCV抗体指数下降不一定意味着与PML风险降低相关。