Heart Research Institute, Charles Perkins Centre, University of Sydney, Camperdown, New South Wales, Australia.
School of Mathematics and Statistics, University of New South Wales, Sydney, Australia.
PLoS Med. 2019 Sep 25;16(9):e1002903. doi: 10.1371/journal.pmed.1002903. eCollection 2019 Sep.
The precise age distribution and calculated stroke risk of screen-detected atrial fibrillation (AF) is not known. Therefore, it is not possible to determine the number needed to screen (NNS) to identify one treatable new AF case (NNS-Rx) (i.e., Class-1 oral anticoagulation [OAC] treatment recommendation) in each age stratum. If the NNS-Rx is known for each age stratum, precise cost-effectiveness and sensitivity simulations can be performed based on the age distribution of the population/region to be screened. Such calculations are required by national authorities and organisations responsible for health system budgets to determine the best age cutoffs for screening programs and decide whether programs of screening should be funded. Therefore, we aimed to determine the exact yield and calculated stroke-risk profile of screen-detected AF and NNS-Rx in 5-year age strata.
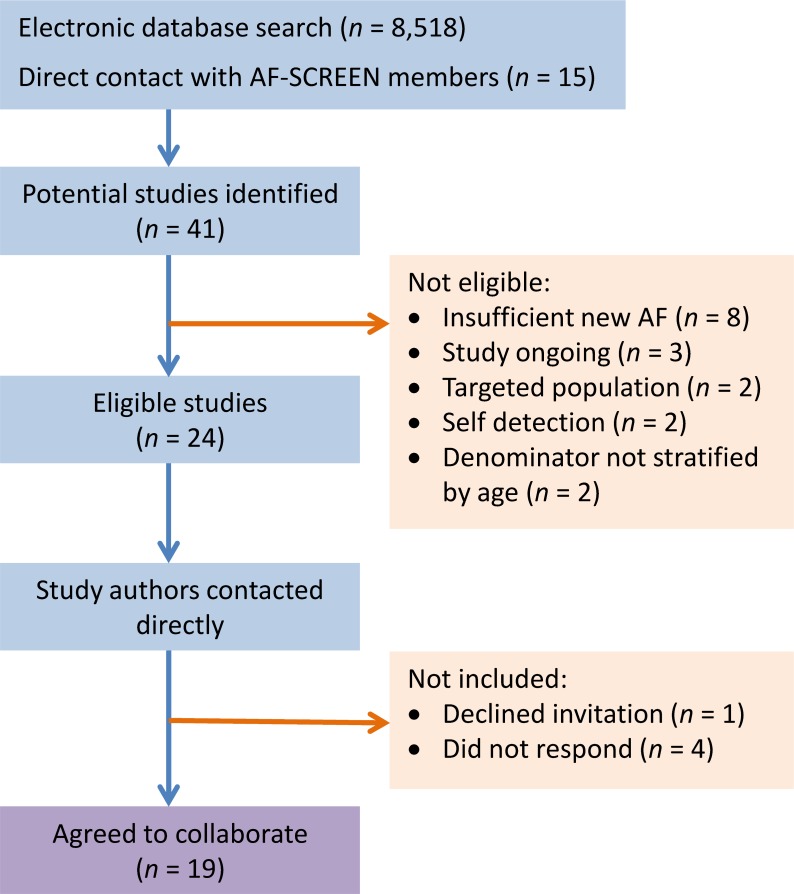
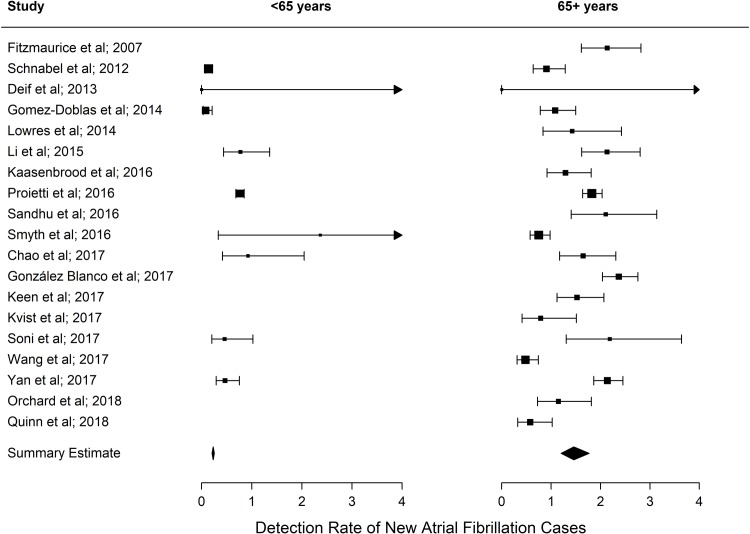
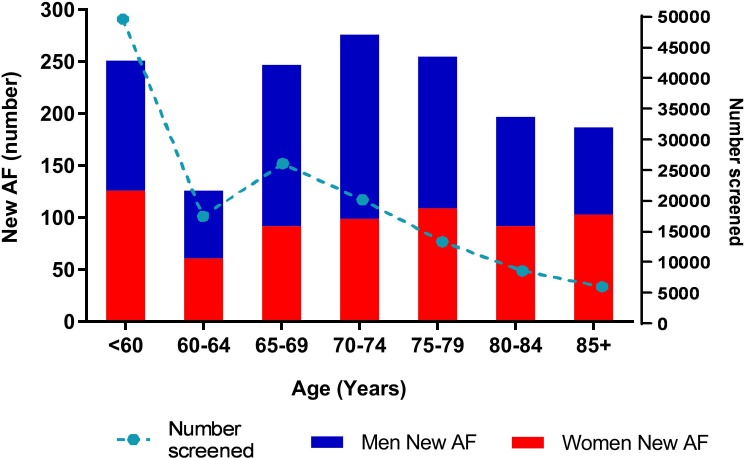
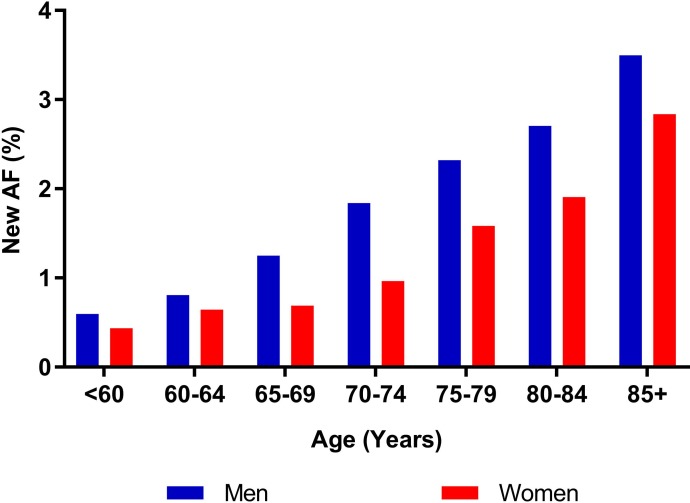
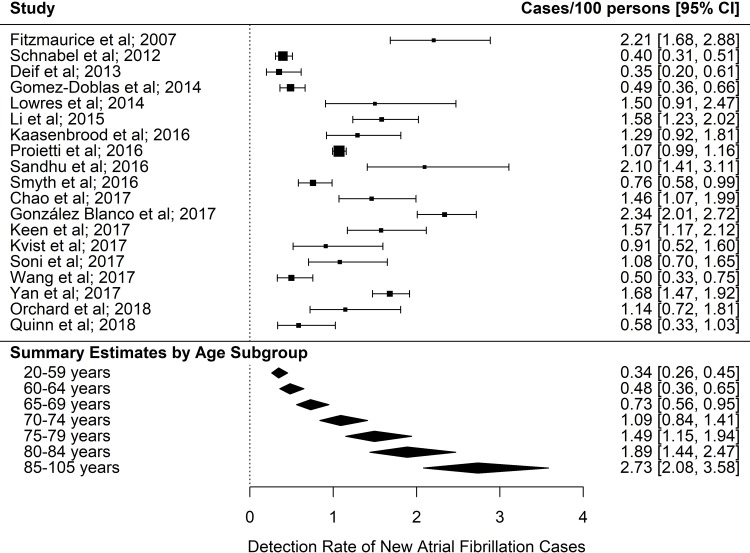
A systematic review of Medline, Pubmed, and Embase was performed (January 2007 to February 2018), and AF-SCREEN international collaboration members were contacted to identify additional studies. Twenty-four eligible studies were identified that performed a single time point screen for AF in a general ambulant population, including people ≥65 years. Authors from eligible studies were invited to collaborate and share patient-level data. Statistical analysis was performed using random effects logistic regression for AF detection rate, and Poisson regression modelling for CHA2DS2-VASc scores. Nineteen studies (14 countries from a mix of low- to middle- and high-income countries) collaborated, with 141,220 participants screened and 1,539 new AF cases. Pooled yield of screening was greater in males across all age strata. The age/sex-adjusted detection rate for screen-detected AF in ≥65-year-olds was 1.44% (95% CI, 1.13%-1.82%) and 0.41% (95% CI, 0.31%-0.53%) for <65-year-olds. New AF detection rate increased progressively with age from 0.34% (<60 years) to 2.73% (≥85 years). Neither the choice of screening methodology or device, the geographical region, nor the screening setting influenced the detection rate of AF. Mean CHA2DS2-VASc scores (n = 1,369) increased with age from 1.1 (<60 years) to 3.9 (≥85 years); 72% of ≥65 years had ≥1 additional stroke risk factor other than age/sex. All new AF ≥75 years and 66% between 65 and 74 years had a Class-1 OAC recommendation. The NNS-Rx is 83 for ≥65 years, 926 for 60-64 years; and 1,089 for <60 years. The main limitation of this study is there are insufficient data on sociodemographic variables of the populations and possible ascertainment biases to explain the variance in the samples.
People with screen-detected AF are at elevated calculated stroke risk: above age 65, the majority have a Class-1 OAC recommendation for stroke prevention, and >70% have ≥1 additional stroke risk factor other than age/sex. Our data, based on the largest number of screen-detected AF collected to date, show the precise relationship between yield and estimated stroke risk profile with age, and strong dependence for NNS-RX on the age distribution of the population to be screened: essential information for precise cost-effectiveness calculations.
目前尚不清楚经筛查发现的心房颤动(房颤)的确切年龄分布和计算出的中风风险。因此,无法确定每个年龄组的筛查所需人数(NNS),以识别每个年龄组中可治疗的新房颤病例(NNS-Rx)(即,I 类口服抗凝剂[OAC]治疗推荐)。如果每个年龄组的 NNS-Rx 已知,则可以根据要筛查的人群/地区的年龄分布进行精确的成本效益和敏感性模拟。负责卫生系统预算的国家当局和组织需要进行此类计算,以确定筛查计划的最佳年龄截止值,并决定是否应资助筛查计划。因此,我们旨在确定经筛查发现的房颤的确切检出率和计算出的中风风险特征,并按 5 年年龄组进行分析。
对 Medline、Pubmed 和 Embase 进行了系统评价(2007 年 1 月至 2018 年 2 月),并联系了 AF-SCREEN 国际合作成员以确定其他研究。确定了 24 项符合条件的研究,这些研究在一般的门诊人群中进行了单次房颤筛查,包括年龄≥65 岁的人群。邀请符合条件的研究的作者进行合作并共享患者水平数据。使用随机效应逻辑回归分析房颤检出率,使用泊松回归模型分析 CHA2DS2-VASc 评分。来自 19 项研究(来自中低收入和高收入国家的 14 个国家)的 141220 名参与者进行了筛查,共检出 1539 例新房颤病例。在所有年龄组中,男性筛查检出率均较高。≥65 岁人群中,年龄/性别校正后的房颤检出率为 1.44%(95%CI,1.13%-1.82%),<65 岁人群为 0.41%(95%CI,0.31%-0.53%)。新房颤检出率随着年龄的增长而逐渐增加,从 0.34%(<60 岁)增加到 2.73%(≥85 岁)。筛查方法或设备的选择、地理位置或筛查环境均不影响房颤的检出率。平均 CHA2DS2-VASc 评分(n=1369)随着年龄的增长从 1.1(<60 岁)增加到 3.9(≥85 岁);≥65 岁的人群中,72%有除年龄/性别以外的其他一个或多个中风危险因素。≥75 岁的所有新房颤和 65-74 岁之间的 66%患者有 I 类 OAC 治疗推荐。NNS-Rx 为≥65 岁为 83,60-64 岁为 926,<60 岁为 1089。本研究的主要局限性是缺乏有关人群社会人口统计学变量的充分数据,以及可能存在的确定偏差,无法解释样本中的差异。
经筛查发现的房颤患者具有较高的计算出的中风风险:≥65 岁时,大多数患者有 I 类 OAC 预防中风的推荐,超过 70%的患者除年龄/性别以外还有其他一个或多个中风危险因素。我们的数据基于迄今为止收集的最大数量的经筛查发现的房颤病例,显示了检出率与估计中风风险特征与年龄之间的精确关系,以及 NNS-Rx 强烈依赖于要筛查的人群的年龄分布:这是精确进行成本效益计算的重要信息。