Department of Surgical Sciences, Uppsala University, 751 85, Uppsala, Sweden.
Division of Surgery, CLINTEC, Karolinska Institutet, Center for Digestive Diseases, Karolinska University Hospital, Stockholm, Sweden.
Surg Endosc. 2020 May;34(5):1939-1947. doi: 10.1007/s00464-019-06966-w. Epub 2019 Sep 26.
Perforations related to endoscopic retrograde cholangiopancreatography (ERCP) are rare but feared adverse events with highly reported morbidity and mortality rates. The aim was to evaluate the incidence and outcome of ERCP-related perforations and to identify risk factors for death due to perforations in a population-based study.
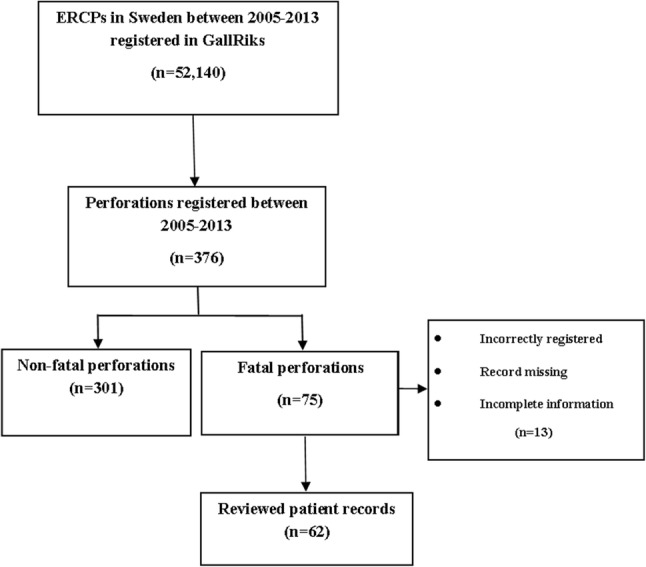
Between May 2005 and December 2013, a total of 52,140 ERCPs were registered in GallRiks, a Swedish nationwide, population-based registry. A total of 376 (0.72%) were registered as perforations or extravasation of contrast during ERCP or as perforation in the 30-day follow-up. The patients with perforation were divided into fatal and non-fatal groups and analyzed for mortality risk factors. The case volume of centers and endoscopists were divided into the upper quartile (Q4) and the lower three quartile (Q1-3) groups. Furthermore, fatal group patients' records were reviewed.
Death within 90 days after ERCP-related perforations or at the index hospitalization occurred in 20% (75 out of 376) for all perforations and 0.1% (75 out of 52,140) for all ERCPs. The independent risk factors for death after perforation were malignancy (OR 11.2, 95% CI 5.8-21.6), age over 80 years (OR 3.8, 95% CI 2.0-7.4), and sphincterotomy in the pancreatic duct (OR 2.8, 95% CI 1.1-7.5). In Q4 centers, the mortality was similar with or without pancreatic duct sphincterotomy (14% vs. 13%, p = 1.0), but in Q1-3 centers mortality was higher (45% vs. 21%, p = 0.024).
ERCP-related perforations are severe adverse events with low incidence (0.7%) and high mortality rate up to 20%. Malignancy, age over 80 years, and sphincterotomy in the pancreatic duct increase the risk to die after a perforation. The risk of a fatal outcome in perforations after pancreatic duct sphincterotomy was reduced when occurred at a Q4-center. In the case of a complicated perforation a transfer to a Q4-center may be considered.
内镜逆行胰胆管造影(ERCP)相关穿孔是罕见但令人恐惧的不良事件,其发病率和死亡率均有较高报道。本研究旨在评估基于人群的 ERCP 相关穿孔的发生率和结局,并确定因穿孔导致死亡的危险因素。
在 2005 年 5 月至 2013 年 12 月期间,在瑞典全国性基于人群的 GallRiks 注册中心共登记了 52140 例 ERCP。共有 376 例(0.72%)在 ERCP 期间或在 30 天随访期间被登记为穿孔或造影剂外渗,或穿孔。将穿孔患者分为致命组和非致命组,并分析死亡率的危险因素。中心和内镜医生的例数被分为上四分位数(Q4)和下三分位数(Q1-3)组。此外,还对致命组患者的记录进行了回顾。
所有穿孔患者中有 20%(75 例)在 ERCP 相关穿孔后 90 天内或在指数住院期间死亡,所有 ERCP 患者中有 0.1%(75 例)死亡。穿孔后死亡的独立危险因素包括恶性肿瘤(OR 11.2,95%CI 5.8-21.6)、年龄超过 80 岁(OR 3.8,95%CI 2.0-7.4)和胰管括约肌切开术(OR 2.8,95%CI 1.1-7.5)。在 Q4 中心,行或不行胰管括约肌切开术的死亡率相似(14%比 13%,p=1.0),但在 Q1-3 中心,死亡率更高(45%比 21%,p=0.024)。
ERCP 相关穿孔是一种严重的不良事件,发生率较低(0.7%),死亡率高达 20%。恶性肿瘤、年龄超过 80 岁和胰管括约肌切开术增加了穿孔后死亡的风险。在 Q4 中心进行胰管括约肌切开术的穿孔患者,其致命结局的风险降低。在发生复杂穿孔的情况下,可考虑将患者转至 Q4 中心。