Cartes d'Identité des Tumeurs (CIT) Program, Ligue Nationale Contre le Cancer, Paris, France.
Cartes d'Identité des Tumeurs (CIT) Program, Ligue Nationale Contre le Cancer, Paris, France.
Eur Urol. 2020 Apr;77(4):420-433. doi: 10.1016/j.eururo.2019.09.006. Epub 2019 Sep 26.
Muscle-invasive bladder cancer (MIBC) is a molecularly diverse disease with heterogeneous clinical outcomes. Several molecular classifications have been proposed, but the diversity of their subtype sets impedes their clinical application.
To achieve an international consensus on MIBC molecular subtypes that reconciles the published classification schemes.
DESIGN, SETTING, AND PARTICIPANTS: We used 1750 MIBC transcriptomic profiles from 16 published datasets and two additional cohorts.
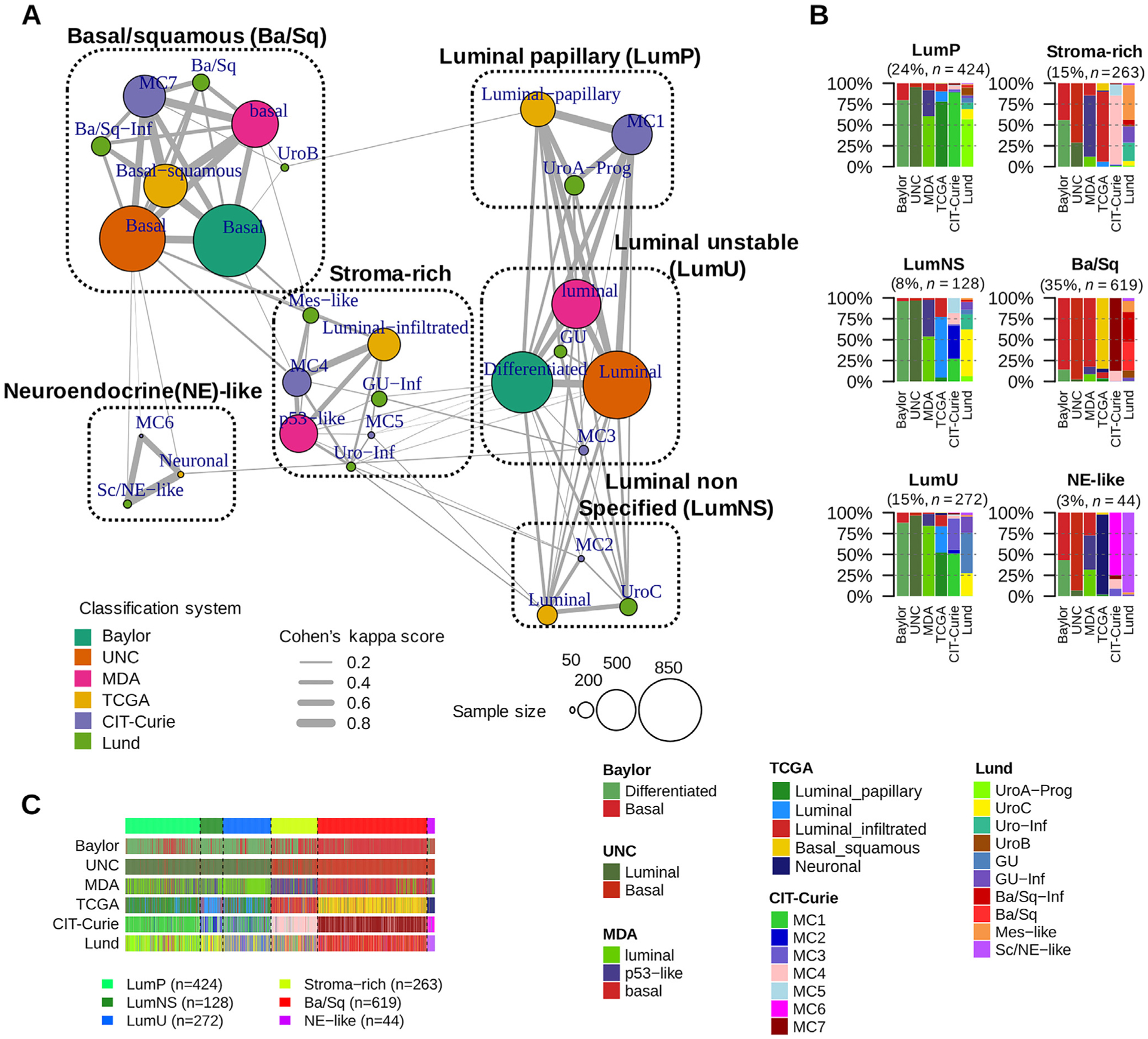
We performed a network-based analysis of six independent MIBC classification systems to identify a consensus set of molecular classes. Association with survival was assessed using multivariable Cox models.
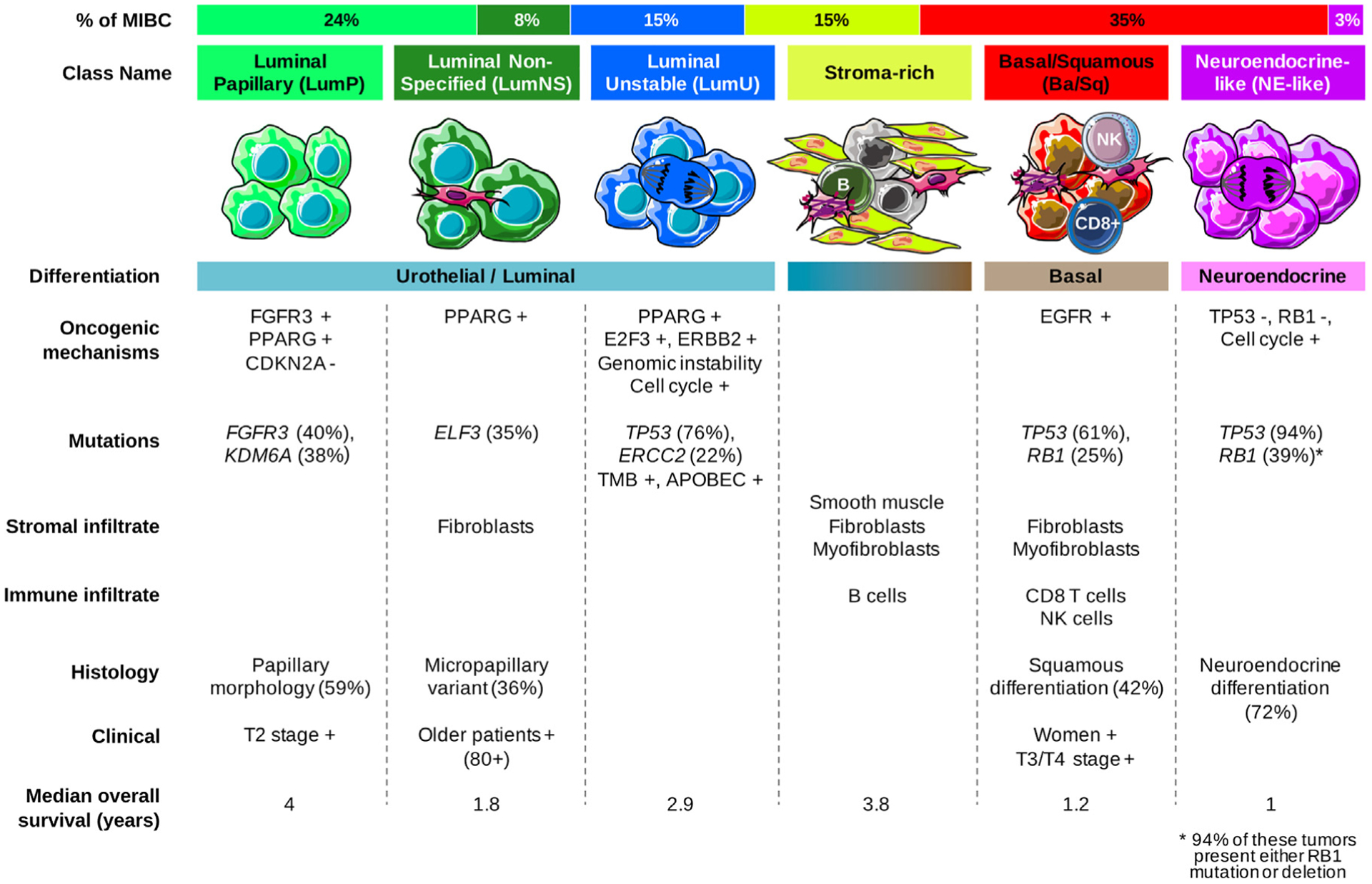
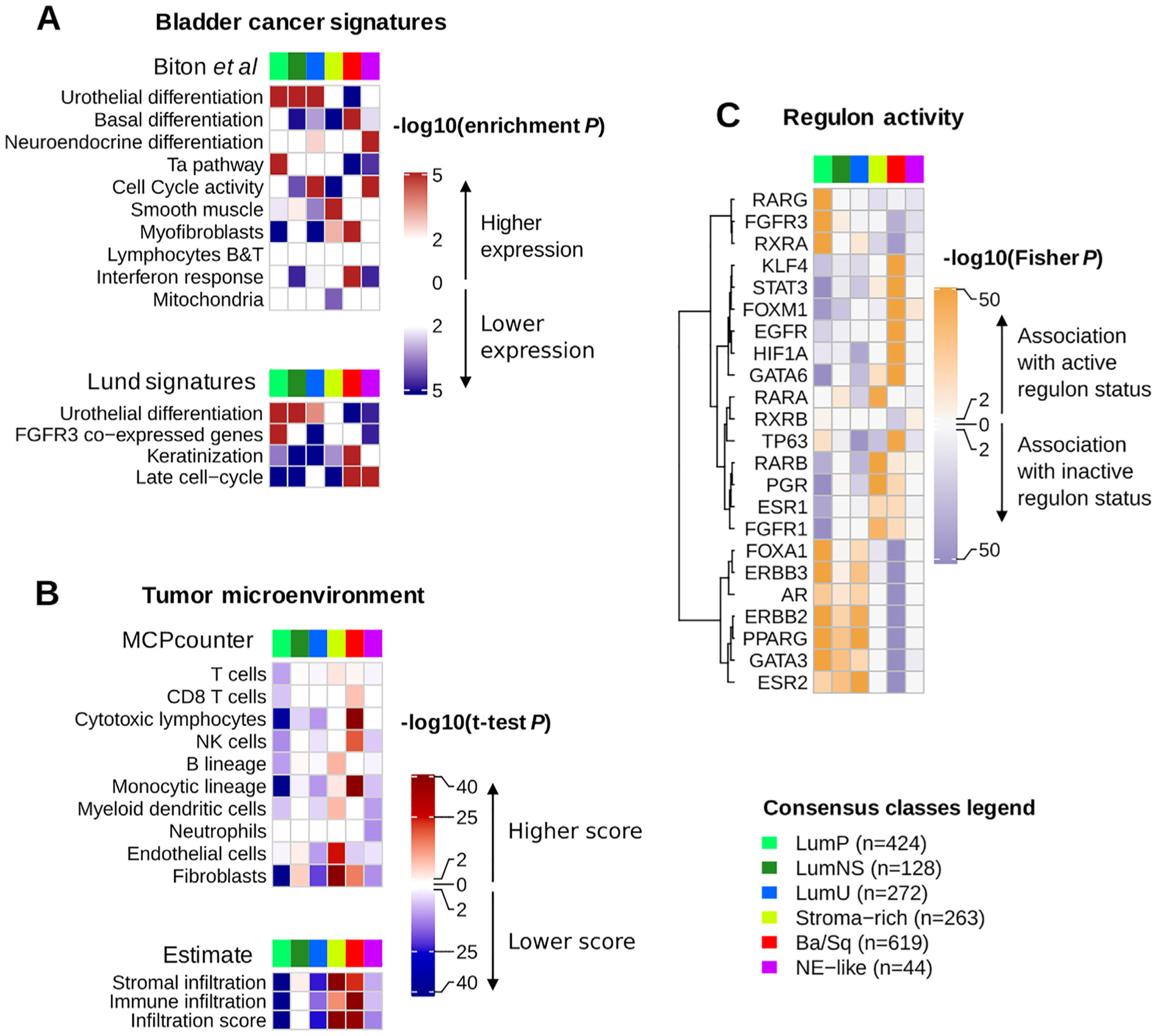
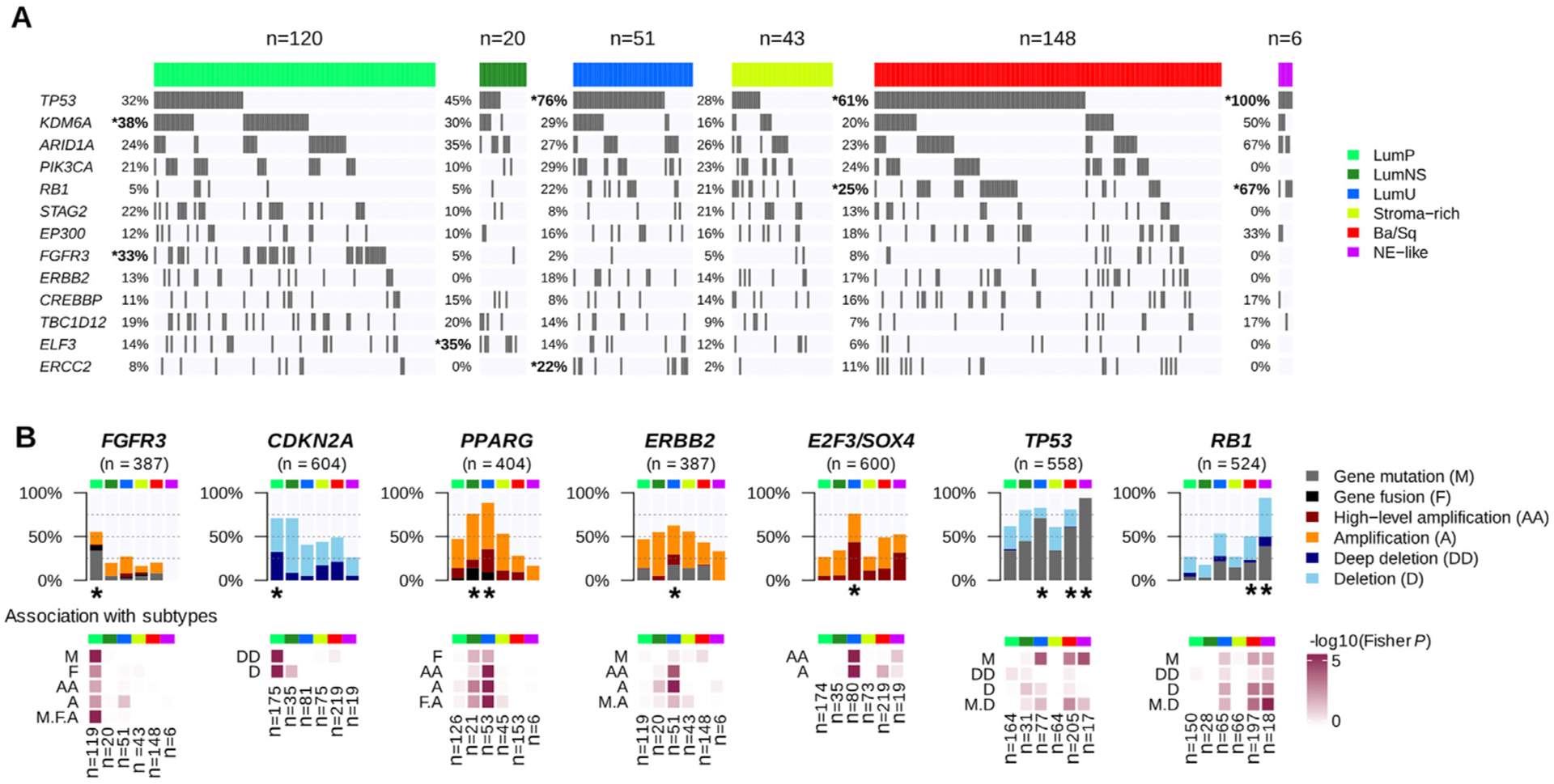
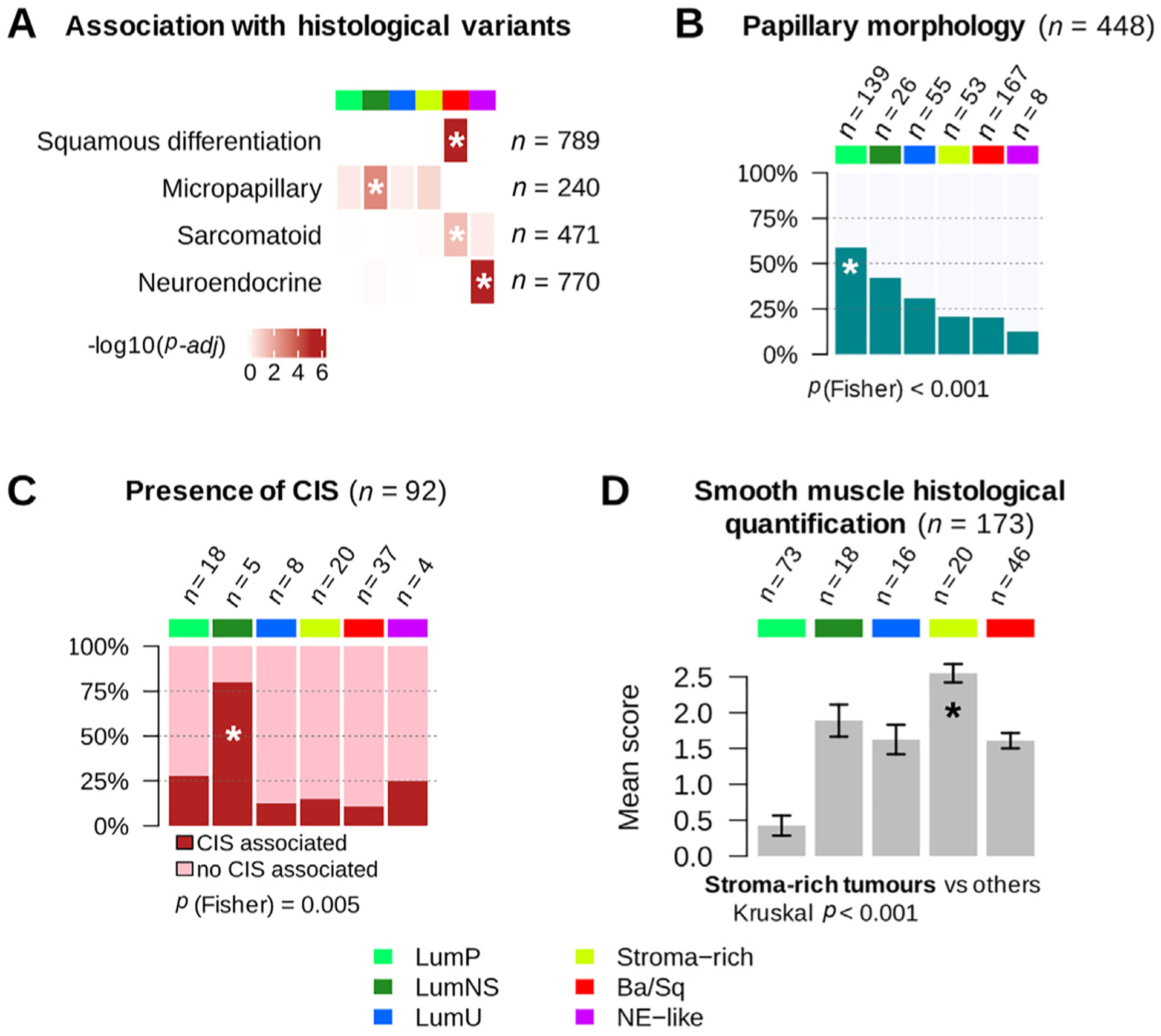
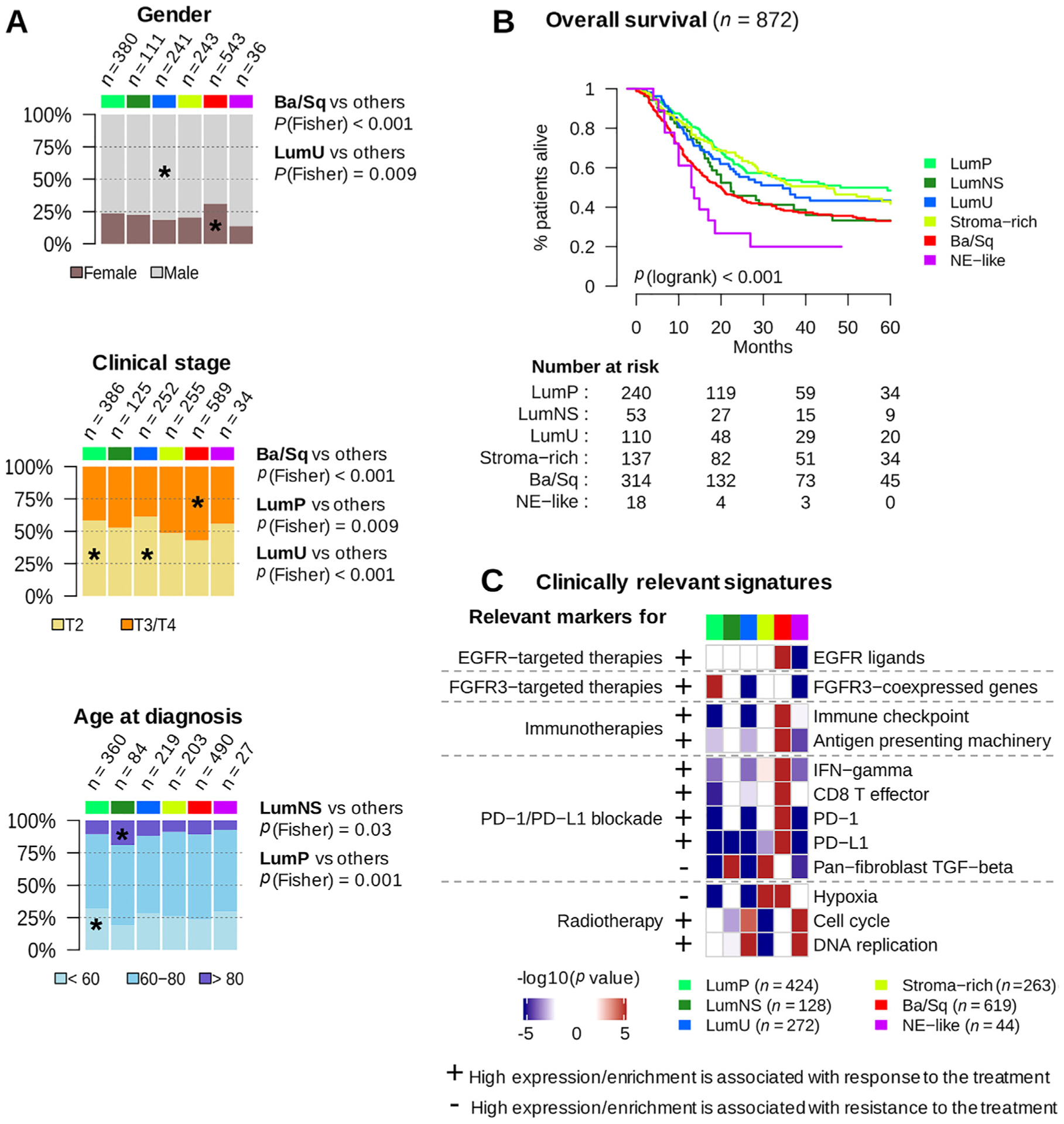
We report the results of an international effort to reach a consensus on MIBC molecular subtypes. We identified a consensus set of six molecular classes: luminal papillary (24%), luminal nonspecified (8%), luminal unstable (15%), stroma-rich (15%), basal/squamous (35%), and neuroendocrine-like (3%). These consensus classes differ regarding underlying oncogenic mechanisms, infiltration by immune and stromal cells, and histological and clinical characteristics, including outcomes. We provide a single-sample classifier that assigns a consensus class label to a tumor sample's transcriptome. Limitations of the work are retrospective clinical data collection and a lack of complete information regarding patient treatment.
This consensus system offers a robust framework that will enable testing and validation of predictive biomarkers in future prospective clinical trials.
Bladder cancers are heterogeneous at the molecular level, and scientists have proposed several classifications into sets of molecular classes. While these classifications may be useful to stratify patients for prognosis or response to treatment, a consensus classification would facilitate the clinical use of molecular classes. Conducted by multidisciplinary expert teams in the field, this study proposes such a consensus and provides a tool for applying the consensus classification in the clinical setting.
肌层浸润性膀胱癌(MIBC)是一种分子多样性疾病,具有异质性的临床结局。已经提出了几种分子分类,但它们的亚型集的多样性阻碍了它们的临床应用。
达成 MIBC 分子亚型的国际共识,协调已发表的分类方案。
设计、设置和参与者:我们使用了来自 16 个已发表数据集和两个额外队列的 1750 个 MIBC 转录组谱。
我们对六个独立的 MIBC 分类系统进行了基于网络的分析,以确定一组共识的分子类别。使用多变量 Cox 模型评估与生存的关联。
我们报告了一项国际努力达成 MIBC 分子亚型共识的结果。我们确定了一组共识的六个分子类别:亮细胞乳头状(24%)、亮细胞非特指(8%)、亮细胞不稳定(15%)、基质丰富(15%)、基底/鳞状(35%)和神经内分泌样(3%)。这些共识类别在潜在的致癌机制、免疫和基质细胞浸润以及组织学和临床特征(包括结局)方面存在差异。我们提供了一个单样本分类器,可将共识类别标签分配给肿瘤样本的转录组。该工作的局限性在于回顾性临床数据收集和缺乏关于患者治疗的完整信息。
该共识系统提供了一个强大的框架,将能够在未来的前瞻性临床试验中测试和验证预测生物标志物。
膀胱癌在分子水平上具有异质性,科学家已经提出了几种分类方法,将其分为分子类别。虽然这些分类方法可能有助于对预后或治疗反应进行分层,但共识分类将有助于分子类别的临床应用。该研究由该领域的多学科专家团队进行,提出了这样一种共识,并提供了一种在临床环境中应用共识分类的工具。