Geriatrics Research, Education and Clinical Center (GRECC), Miami VA Healthcare System, 1201 NW 16th St., 11 GRC, CLC 207 A2, Miami, FL, 33125, USA.
Department of Humanities, Health and Society, Florida International University Herbert Wertheim College of Medicine, Miami, FL, 33199, USA.
Drugs Aging. 2019 Dec;36(12):1083-1096. doi: 10.1007/s40266-019-00706-4.
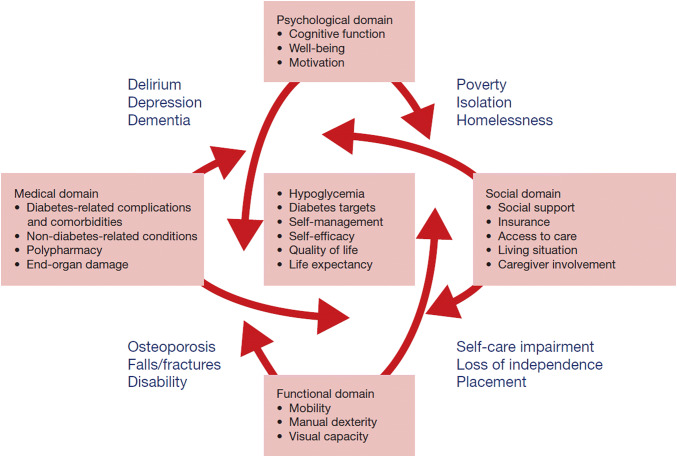
The management of type 2 diabetes mellitus in older adults requires a comprehensive understanding of the relationship between the disease (medical) and the functional, psychological/cognitive, and social geriatric domains, to individualize both glycemic targets and therapeutic approaches. Prevention of hypoglycemia is a major priority that should be addressed as soon as its presence or risk is detected, adjusting the target and therapeutics accordingly. Nonetheless, treatment intensification should not be neglected when applicable, consistent with recommendations from organizations such as the American Geriatrics Society and the American Diabetes Association, to reduce not only long-term macrovascular and microvascular complications (individualization), but also short-term complications from hyperglycemia (polyuria, volume depletion, urinary incontinence). Such complications can negatively impact the physical and cognitive function of older adults, worsen their quality of life, and additionally affect their families and society. We emphasize individualization, utilizing the multiple classes of antihyperglycemic agents available. Metformin remains as first-line therapy, and additional agents offer advantages and disadvantages that ought to be considered when developing a patient-centric plan of care. For selected cases, injectable therapies such as long-acting basal insulin analogs and glucagon-like peptide-1 receptor agonists can offer advantages to counter hypoglycemia risk, patient-related barriers, and clinical inertia. Furthermore, some injectable agents could potentially simplify regimens while providing safe and effective glycemic control. In this review, we discuss the use of injectable therapies for selected community-dwelling older adults, barriers to transition to injectable therapy, and measures aimed at removing these barriers and assisting physicians and their teams to transition older patients to injectable therapies when appropriate.
2 型糖尿病在老年人中的管理需要全面了解疾病(医学)与功能、心理/认知和社会老年领域之间的关系,以便个体化血糖目标和治疗方法。预防低血糖是一个主要重点,一旦发现或存在低血糖风险,就应加以解决,相应调整目标和治疗方法。然而,在适用的情况下,不应忽视治疗强化,这符合美国老年学会和美国糖尿病协会等组织的建议,以减少不仅是长期大血管和微血管并发症(个体化),还有短期高血糖并发症(多尿、容量不足、尿失禁)。这些并发症会对老年人的身体和认知功能产生负面影响,降低他们的生活质量,并对他们的家庭和社会产生额外影响。我们强调个体化,利用多种类的抗高血糖药物。二甲双胍仍然是一线治疗药物,其他药物具有优缺点,在制定以患者为中心的护理计划时应加以考虑。对于选定的病例,长效基础胰岛素类似物和胰高血糖素样肽-1 受体激动剂等注射疗法可以提供优势,以应对低血糖风险、患者相关障碍和临床惰性。此外,一些注射剂可能具有简化方案的潜力,同时提供安全有效的血糖控制。在这篇综述中,我们讨论了为选定的社区居住老年人使用注射疗法、向注射疗法过渡的障碍,以及旨在消除这些障碍并帮助医生及其团队在适当情况下为老年患者过渡到注射疗法的措施。