Division of Medical Oncology and Hematology, Princess Margaret Cancer Centre, University Health Network, Toronto, Ontario, Canada.
Department of Medicine, University of Toronto, Toronto, Ontario, Canada.
JAMA Netw Open. 2019 Oct 2;2(10):e1912823. doi: 10.1001/jamanetworkopen.2019.12823.
Emergency department visits and hospitalizations after starting systemic therapy for cancer are frequent, undesirable, and costly. A score to quantify the risk of needing acute care can inform decision-making and facilitate the development of preventive interventions.
To develop and validate a score to predict early use of acute care after initiating systemic therapy for cancer.
DESIGN, SETTING, AND PARTICIPANTS: A retrospective population-based cohort study was conducted between July 1, 2014, and June 30, 2015. Patients with cancer were eligible if they started a new systemic therapy for cancer, regardless of line of therapy. A total of 12 162 patients in Southwestern Ontario, Canada, formed the development cohort and 15 845 patients in Northeastern Ontario formed the validation cohort. Data analysis was conducted from December 1, 2016, to August 10, 2019.
The Prediction of Acute Care Use During Cancer Treatment (PROACCT) score was created based on logistic regression in the development cohort. Combinations of cancer type and regimens were grouped into quintiles based on risk of needing acute care. The score was assessed in the validation cohort.
At least 1 emergency department visit or hospitalization within 30 days after starting systemic therapy for cancer identified from administrative databases.
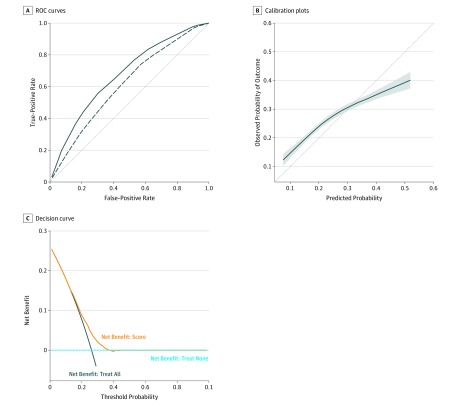
Among the 12 162 patients in the development cohort, 6903 were women and 5259 were men (mean [SD] age, 62.9 [12.6] years); among the 15 845 patients in the validation cohort, 9025 were women and 6820 were men (mean [SD] age, 62.9 [12.6] years). Use of acute care occurred within 30 days after initiation of systemic therapy in 3039 patients (25.0%) in the development cohort and 4212 patients (26.6%) in the validation cohort. Three characteristics predicted early use of acute care and formed the PROACCT score: combination of cancer type and treatment regimen, age, and emergency department visits in the prior year (C statistic, 0.67; 95% CI, 0.66-0.69; P < .001). Other characteristics including patient-reported symptoms did not improve performance. In the validation cohort, the PROACCT score was associated with use of acute care (odds ratio per point increase, 1.22; 95% CI, 1.20-1.24; P < .001), had a C statistic of 0.61 (95% CI, 0.60-0.62; P < .001), was reasonably calibrated, and provided net benefit in decision curve analysis.
The PROACCT score predicted the risk of early use of acute care in patients starting systemic treatment for cancer and could be incorporated at the point of care to select patients for preventive interventions. Future studies should validate the PROACCT score in other settings.
癌症患者开始接受全身治疗后,频繁出现急诊就诊和住院治疗的情况,这不仅不令人满意,还耗费了大量医疗资源。一个可以量化急性护理需求风险的评分可以为决策提供信息,并有助于制定预防干预措施。
开发和验证一个预测癌症患者开始全身治疗后早期需要急性护理的评分。
设计、地点和参与者:这是一项回顾性基于人群的队列研究,于 2014 年 7 月 1 日至 2015 年 6 月 30 日进行。如果患者开始新的全身治疗,无论治疗线数如何,均有资格入选。加拿大安大略省西南部的 12162 名患者组成了开发队列,安大略省东北部的 15845 名患者组成了验证队列。数据分析于 2016 年 12 月 1 日至 2019 年 8 月 10 日进行。
PROACCT 评分是根据开发队列中的逻辑回归创建的。根据需要急性护理的风险,将癌症类型和方案的组合分为五组。在验证队列中评估了该评分。
从行政数据库中确定癌症患者开始全身治疗后 30 天内至少有 1 次急诊就诊或住院治疗。
在开发队列的 12162 名患者中,6903 名为女性,5259 名为男性(平均[SD]年龄,62.9[12.6]岁);在验证队列的 15845 名患者中,9025 名为女性,6820 名为男性(平均[SD]年龄,62.9[12.6]岁)。在开发队列中,有 3039 名(25.0%)患者在开始全身治疗后 30 天内使用了急性护理,在验证队列中有 4212 名(26.6%)患者使用了急性护理。三个特征预测了早期使用急性护理,并构成了 PROACCT 评分:癌症类型和治疗方案的组合、年龄和前一年的急诊就诊(C 统计量,0.67;95%CI,0.66-0.69;P<0.001)。其他特征,包括患者报告的症状,并没有改善评分的性能。在验证队列中,PROACCT 评分与急性护理的使用相关(每增加 1 分的比值比,1.22;95%CI,1.20-1.24;P<0.001),C 统计量为 0.61(95%CI,0.60-0.62;P<0.001),具有较好的校准度,并在决策曲线分析中提供了净收益。
PROACCT 评分预测了癌症患者开始全身治疗后早期使用急性护理的风险,可以在护理点纳入该评分,以选择需要预防干预的患者。未来的研究应该在其他环境中验证 PROACCT 评分。