Asban Ammar, Chung Sebastian K, Xie Rongbing, Lindeman Brenessa M, Balentine Courtney J, Kirklin James K, Chen Herbert
Department of Surgery, The University of Alabama at Birmingham, Birmingham, AL, USA.
Kirklin Institute for Research in Surgical Outcomes, Department of Surgery, The University of Alabama at Birmingham, Birmingham, AL, USA.
Clin Med Insights Endocrinol Diabetes. 2019 Sep 25;12:1179551419866196. doi: 10.1177/1179551419866196. eCollection 2019.
Demographic disparities have been described for survival after thyroid cancer surgery using national registries and databases. At the institution level, we hypothesized that assessing survival after thyroid cancer surgery in a long-term cohort with diverse gender and racial groups would reveal disparities in survival.
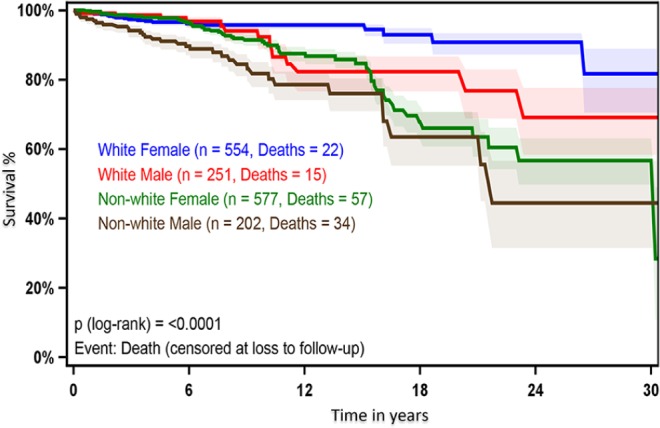
We examined medical records of patients with papillary or follicular thyroid cancer undergoing thyroidectomy, lobectomy, and other surgical procedures from 1971 to 2016 at a tertiary referral center. We obtained information on demographics, cancer stage, procedure, and radioactive iodine (RAI). We measured survival using Kaplan-Meier estimates and Cox proportional hazards models.
A total of 1440 (91%) patients with papillary cancer and 144 (9%) patients with follicular thyroid cancer underwent total thyroidectomy (1297, 82%), lobectomy (261, 16.5%), and other surgical procedures (26, 1.5%). Most patients (1131, 71%) were woman, and 909 (57%) were older than 45 years. Race/ethnicity included 805 (51%) white, 161 (10%) African Americans, and 618 (39%) other race/ethnicities. Both 10- and 20-year survival rates in nonwhite males were worse compared with nonwhite females ( < .0001). After controlling for age, cancer type, stage, surgical procedure, RAI, and year of surgery, nonwhite males had a higher mortality risk compared with nonwhite females ( = .0376, confidence interval (CI): 1.03-2.43), white males ( < .0001, CI: 1.88-6.54), and white females ( < .0001, CI: 3.31-9.90).
Our diverse cohort demonstrates significant gender and racial disparities in survival after thyroid cancer surgery. To improve health outcomes and reduce health disparities among nonwhite males, interventions and long-term care management should target potentially modifiable causes of worse outcomes in this group.
利用国家登记处和数据库对甲状腺癌手术后的生存率进行了人口统计学差异描述。在机构层面,我们假设在一个包含不同性别和种族群体的长期队列中评估甲状腺癌手术后的生存率会揭示出生存差异。
我们检查了1971年至2016年在一家三级转诊中心接受甲状腺切除术、叶切除术和其他手术的乳头状或滤泡状甲状腺癌患者的病历。我们获取了有关人口统计学、癌症分期、手术程序和放射性碘(RAI)的信息。我们使用Kaplan-Meier估计值和Cox比例风险模型来测量生存率。
共有1440例(91%)乳头状癌患者和144例(9%)滤泡状甲状腺癌患者接受了全甲状腺切除术(1297例,82%)、叶切除术(261例,16.5%)和其他手术(26例,1.5%)。大多数患者(1131例,71%)为女性,909例(57%)年龄超过45岁。种族/族裔包括805例(51%)白人、161例(10%)非裔美国人以及618例(39%)其他种族/族裔。与非白人女性相比,非白人男性的10年和20年生存率均较差(P<0.0001)。在控制了年龄、癌症类型、分期、手术程序、RAI和手术年份后,与非白人女性(P = 0.0376,置信区间(CI):1.03 - 2.43)、白人男性(P<0.0001,CI:1.88 - 6.54)和白人女性(P<0.0001,CI:3.31 - 9.90)相比,非白人男性的死亡风险更高。
我们这个多样化的队列显示了甲状腺癌手术后生存率存在显著的性别和种族差异。为了改善健康结果并减少非白人男性之间的健康差异,干预措施和长期护理管理应针对该群体中可能导致较差结果的可改变原因。