Department of Medicine, Johns Hopkins School of Medicine, 2041 E. Monument Street, Baltimore, MD, 21205, USA.
Immunogenetics Laboratory, 2041 E. Monument Street, Baltimore, MD, 21205, USA.
Pediatr Nephrol. 2020 Jan;35(1):83-94. doi: 10.1007/s00467-019-04344-1. Epub 2019 Oct 10.
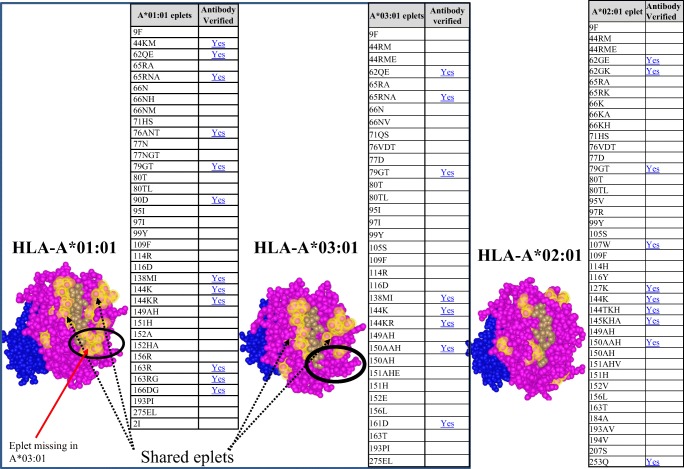
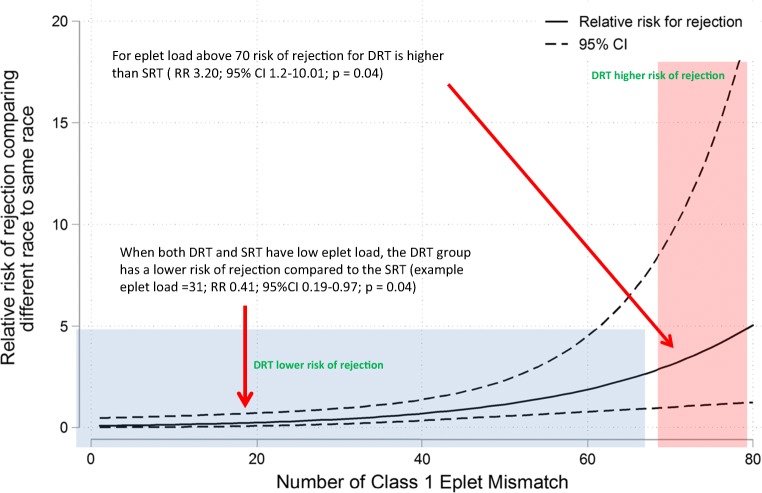
HLA eplet mismatch load has been suggested as an improvement to HLA antigen mismatch determination for organ selection. Given that eplet mismatches are determined based on amino acid sequence difference among HLA alleles, and that the frequency of HLA alleles varies between racial groups, we investigated the correlation between eplet mismatch load and allograft outcomes in 110 pediatric kidney transplant recipients who received their first organ from a donor of the same race (SRT) versus a donor of a different race (DRT). Adjusted modified Poisson regression was used to assess the interaction between eplet mismatch load and race mismatch and its effect on outcome. Caucasians and living donor recipients had lower eplet mismatched loads against their donors compared with non-Caucasian and deceased donor recipients. Overall, for the entire population, the risk of de novo HLA-DSA development was significantly increased with higher eplet loads (p < 0.001). Compared with the SRT group, the DRT group had higher eplet loads when compared with their donor, for HLA class I but not HLA class II molecules; however, there was no significant difference in the incidence of de novo HLA-DSA between the 2 groups. The risk of rejection increased significantly for DRT compared with SRT, only when class I eplet load was ≥ 70 (p = 0.04). Together this data show that eplet mismatch load analysis is an effective tool for alloimmune risk assessment. If considered for donor selection, acceptable eplet mismatch loads determined from studies in homogenous populations may restrict transplantation across racially diverse donor and patient groups with no evidence of poor outcome. Therefore, an acceptable eplet mismatch load threshold must consider the heterogeneity of the transplant population.
HLA 表位错配负荷被认为是改善器官选择中 HLA 抗原错配的一种方法。鉴于表位错配是基于 HLA 等位基因之间的氨基酸序列差异来确定的,并且 HLA 等位基因的频率在不同种族群体之间存在差异,我们研究了 110 名接受来自同种族供体(SRT)和不同种族供体(DRT)的同种异体肾移植受者的表位错配负荷与移植物结局之间的相关性。调整后的改良泊松回归用于评估表位错配负荷与种族错配之间的相互作用及其对结局的影响。与非白人和已故供体受者相比,白人和活体供体受者与其供体的表位错配负荷较低。总体而言,对于整个人群,随着表位负荷的增加,新出现的 HLA-DSA 发展的风险显著增加(p<0.001)。与 SRT 组相比,DRT 组与其供体相比,HLA Ⅰ类分子的表位负荷较高,但 HLA-DSA 的发生率在两组之间无显著差异。与 SRT 相比,DRT 组的排斥反应风险显著增加,仅当 I 类表位负荷≥70 时(p=0.04)。总之,这些数据表明表位错配负荷分析是评估同种免疫风险的有效工具。如果考虑用于供者选择,从同质人群研究中确定的可接受的表位错配负荷可能会限制跨种族多样化的供者和患者群体进行移植,而不会导致不良结局的证据。因此,可接受的表位错配负荷阈值必须考虑移植人群的异质性。