University of Washington School of Medicine, Seattle.
Program in Biostatistics and Biomathematics, Fred Hutchinson Cancer Research Center, Seattle, Washington.
JAMA Netw Open. 2019 Oct 2;2(10):e1912597. doi: 10.1001/jamanetworkopen.2019.12597.
Histopathologic criteria have limited diagnostic reliability for a range of cutaneous melanocytic lesions.
To evaluate the association of second-opinion strategies by general pathologists and dermatopathologists with the overall reliability of diagnosis of difficult melanocytic lesions.
DESIGN, SETTING, AND PARTICIPANTS: This diagnostic study used samples from the Melanoma Pathology Study, which comprises 240 melanocytic lesion samples selected from a dermatopathology laboratory in Bellevue, Washington, and represents the full spectrum of lesions from common nevi to invasive melanoma. Five sets of 48 samples were evaluated independently by 187 US pathologists from July 15, 2013, through May 23, 2016. Data analysis was performed from April 2016 through November 2017.
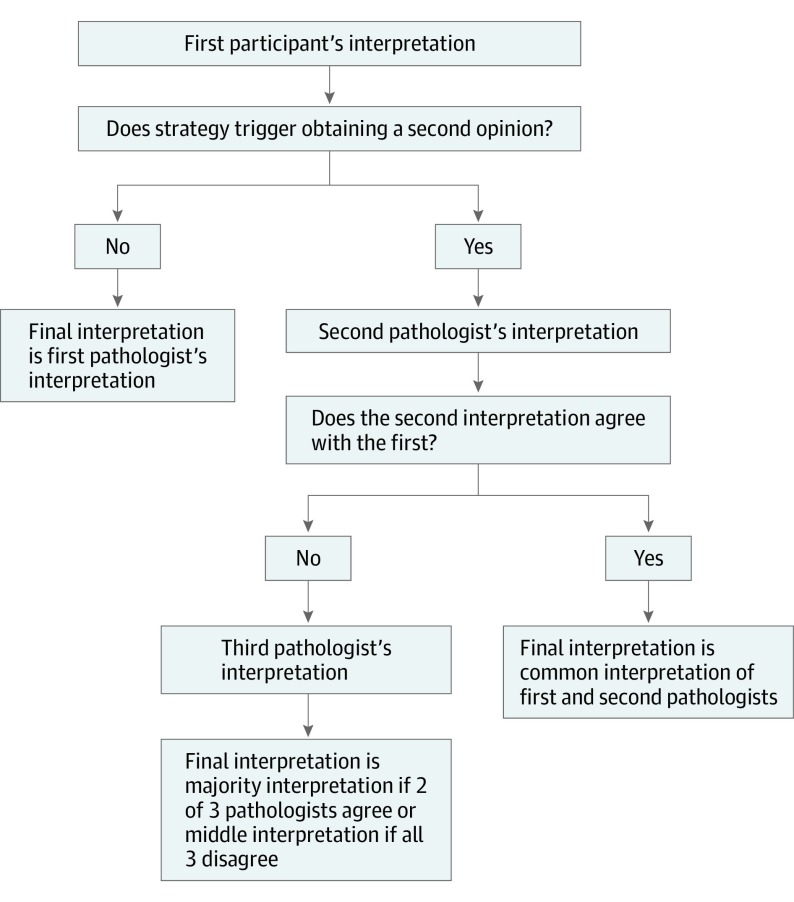
Accuracy of diagnosis, defined as concordance with an expert consensus diagnosis of 3 experienced pathologists, was assessed after applying 10 different second-opinion strategies.
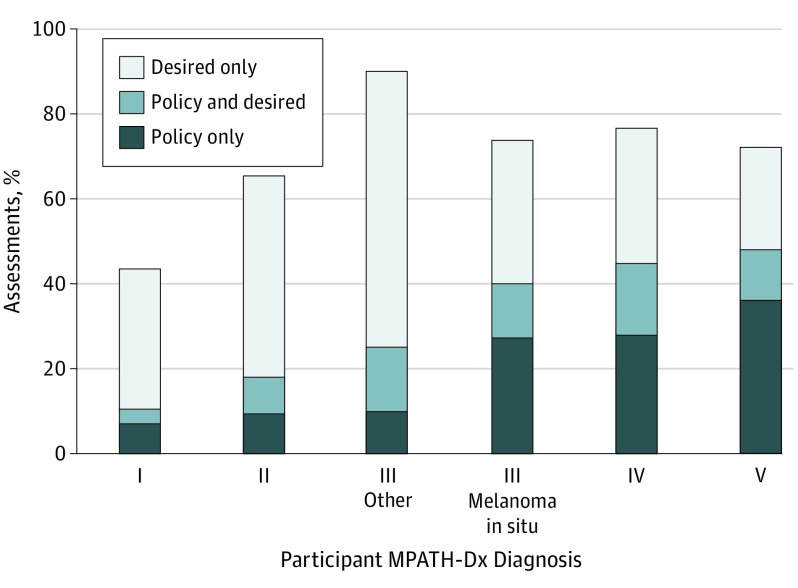
Among the 187 US pathologists examining the 24 lesion samples, 113 were general pathologists (65 men [57.5%]; mean age at survey, 53.7 years [range, 33.0-79.0 years]) and 74 were dermatopathologists (49 men [66.2%]; mean age at survey, 46.4 years [range, 33.0-77.0 years]). Among the 8976 initial case interpretations, physicians desired second opinions for 3899 (43.4%), most often for interpretation of severely dysplastic nevi. The overall misclassification rate was highest when interpretations did not include second opinions and initial reviewers were all general pathologists lacking subspecialty training (52.8%; 95% CI, 51.3%-54.3%). When considering different second opinion strategies, the misclassification of melanocytic lesions was lowest when the first, second, and third consulting reviewers were subspecialty-trained dermatopathologists and when all lesions were subject to second opinions (36.7%; 95% CI, 33.1%-40.7%). When the second opinion strategies were compared with single interpretations without second opinions, the reductions in misclassification rates for some of the strategies were statistically significant, but none of the strategies eliminated diagnostic misclassification. Melanocytic lesions in the middle of the diagnostic spectrum had the highest misclassification rates (eg, moderately or severely dysplastic nevus, Spitz nevus, melanoma in situ, and pathologic stage [p]T1a invasive melanoma). Variability of in situ and thin invasive melanoma was relatively intractable to all examined strategies.
The results of this study suggest that second opinions rendered by dermatopathologists improve reliability of melanocytic lesion diagnosis. However, discordance among pathologists remained high.
组织病理学标准对一系列皮肤黑素细胞病变的诊断可靠性有限。
评估普通病理学家和皮肤病理学家的二次诊断策略与困难黑素细胞病变整体诊断可靠性的关系。
设计、地点和参与者:这项诊断研究使用了来自华盛顿州贝尔维尤皮肤科病理实验室的黑素瘤病理学研究中的样本,包括 240 个黑素细胞病变样本,代表了从常见痣到侵袭性黑色素瘤的所有病变范围。从 2013 年 7 月 15 日至 2016 年 5 月 23 日,5 组 48 个样本由 187 名美国病理学家独立评估。数据分析于 2016 年 4 月至 2017 年 11 月进行。
诊断准确性的定义为与 3 位经验丰富的病理学家共识诊断的一致性,评估了应用 10 种不同的二次诊断策略后的结果。
在检查 24 个病变样本的 187 名美国病理学家中,有 113 名为普通病理学家(65 名男性[57.5%];调查时的平均年龄为 53.7 岁[范围,33.0-79.0 岁]),74 名为皮肤病理学家(49 名男性[66.2%];调查时的平均年龄为 46.4 岁[范围,33.0-77.0 岁])。在 8976 次初始病例解读中,有 3899 次(43.4%)需要二次解读,最常见的是严重发育不良痣的解读。当初始评估者均为缺乏专业培训的普通病理学家且未进行二次评估时,黑素细胞病变的整体错误分类率最高(52.8%;95%CI,51.3%-54.3%)。当考虑不同的二次诊断策略时,当第一、第二和第三会诊病理学家均为专业培训的皮肤科病理学家,且所有病变均接受二次评估时,黑素细胞病变的错误分类最低(36.7%;95%CI,33.1%-40.7%)。与没有二次评估的单一解读相比,当将二次诊断策略与二次诊断策略进行比较时,一些策略的错误分类率降低具有统计学意义,但没有一种策略能够消除诊断错误。位于诊断谱中间的黑素细胞病变的错误分类率最高(例如,中度或重度发育不良痣、Spitz 痣、原位黑色素瘤和病理分期[p]T1a 侵袭性黑色素瘤)。所有检查策略都难以处理处于原位和薄侵袭性黑色素瘤的变异性。
本研究结果表明,皮肤科病理学家提供的二次诊断可提高黑素细胞病变诊断的可靠性。然而,病理学家之间的差异仍然很高。