Jeong Young-Il, Jun In-Gu, Ha Seung-Soo, Kwon Hyun-Jung, Lee Yu-Mi
Department of Anesthesiology and Pain Medicine, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Republic of Korea.
Medicine (Baltimore). 2019 Oct;98(42):e17650. doi: 10.1097/MD.0000000000017650.
Perioperative anesthetic management in cases of severe airway obstruction with positional symptoms can be associated with difficulties in ventilation or intubation, with a risk of acute respiratory decompensation at every stage of anesthesia.
Here we describe the anesthetic management of a 67-year-old man with a massive intrathoracic goiter causing severe tracheal obstruction with positional symptoms. The patient presented with progressive dyspnea that was aggravated in the supine position and was scheduled for total thyroidectomy.
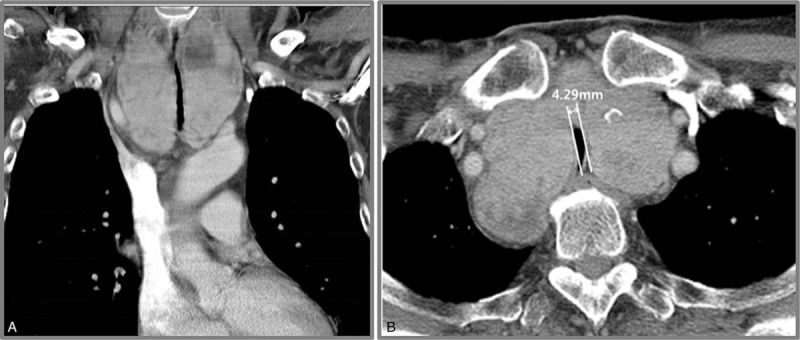
Preoperative computed tomography showed a large goiter extending into the thoracic cavity, with diffuse segmental tracheal narrowing for 6 cm. The diameter at the narrowest portion of the trachea was 4.29 mm.
Before the induction of general anesthesia, we applied extracorporeal membrane oxygenation (ECMO) in preparation for potential difficulties in securing the airway during general anesthesia. Subsequently, anesthesia was successfully induced and maintained.
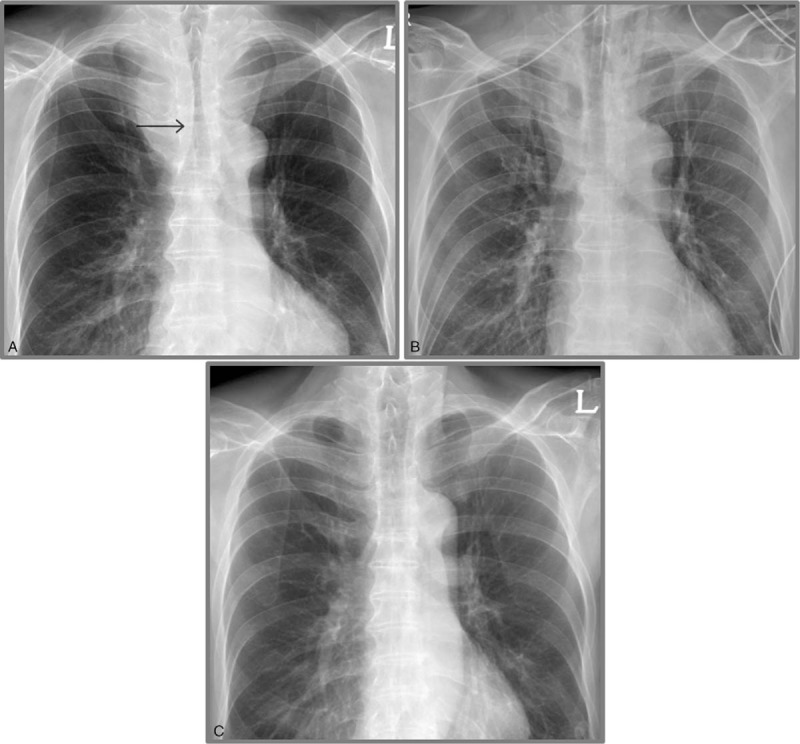
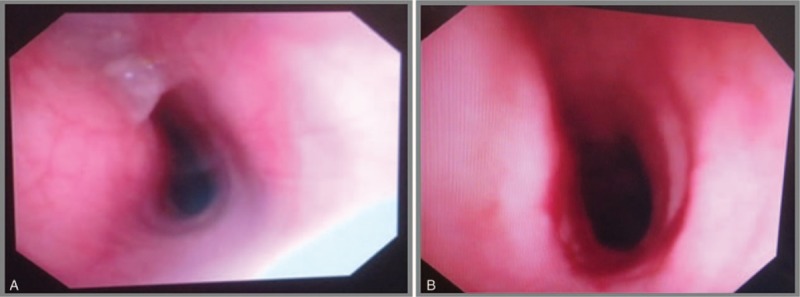
After the surgical procedure, fiberoptic bronchoscopy and chest radiography showed resolution of the tracheal narrowing. ECMO was weaned 2 hours after the surgery, and the patient was extubated on the first postoperative day. He was discharged without any complication.
The findings from this case suggest that the use of ECMO before the induction of general anesthesia is a safe method for maintaining oxygenation in patients with severe tracheal obstruction.
伴有体位性症状的严重气道梗阻患者围手术期麻醉管理可能会出现通气或插管困难,在麻醉的各个阶段都有急性呼吸代偿失调的风险。
在此我们描述一名67岁男性的麻醉管理情况,该患者患有巨大胸内甲状腺肿,导致严重气管梗阻并伴有体位性症状。患者表现为进行性呼吸困难,仰卧位时加重,计划行全甲状腺切除术。
术前计算机断层扫描显示一个巨大甲状腺肿延伸至胸腔,气管弥漫性节段性狭窄6厘米。气管最窄处直径为4.29毫米。
在全身麻醉诱导前,我们应用体外膜肺氧合(ECMO),为全身麻醉期间确保气道安全时可能出现的困难做准备。随后,麻醉诱导和维持均成功。
手术后,纤维支气管镜检查和胸部X线摄影显示气管狭窄缓解。术后2小时停用ECMO,患者于术后第一天拔管。他出院时无任何并发症。
该病例的结果表明,在全身麻醉诱导前使用ECMO是维持严重气管梗阻患者氧合的一种安全方法。