Mike and Valeria Rosenbloom Centre for Cardiovascular Prevention, Department of Medicine, McGill University Health Centre, Montreal, Quebec, Canada.
Monash Health Centre, Victoria, Australia.
JAMA Cardiol. 2019 Dec 1;4(12):1287-1295. doi: 10.1001/jamacardio.2019.3780.
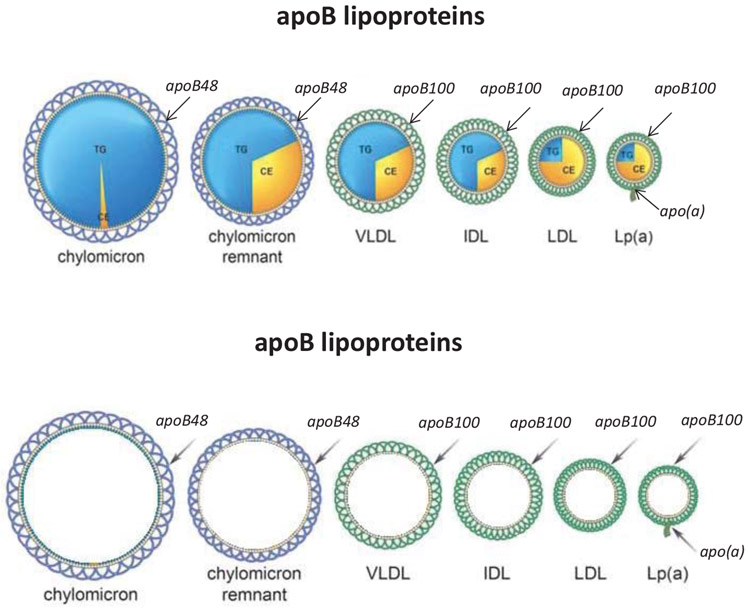
The conventional model of atherosclerosis presumes that the mass of cholesterol within very low-density lipoprotein particles, low-density lipoprotein particles, chylomicron, and lipoprotein (a) particles in plasma is the principal determinant of the mass of cholesterol that will be deposited within the arterial wall and will drive atherogenesis. However, each of these particles contains one molecule of apolipoprotein B (apoB) and there is now substantial evidence that apoB more accurately measures the atherogenic risk owing to the apoB lipoproteins than does low-density lipoprotein cholesterol or non-high-density lipoprotein cholesterol.
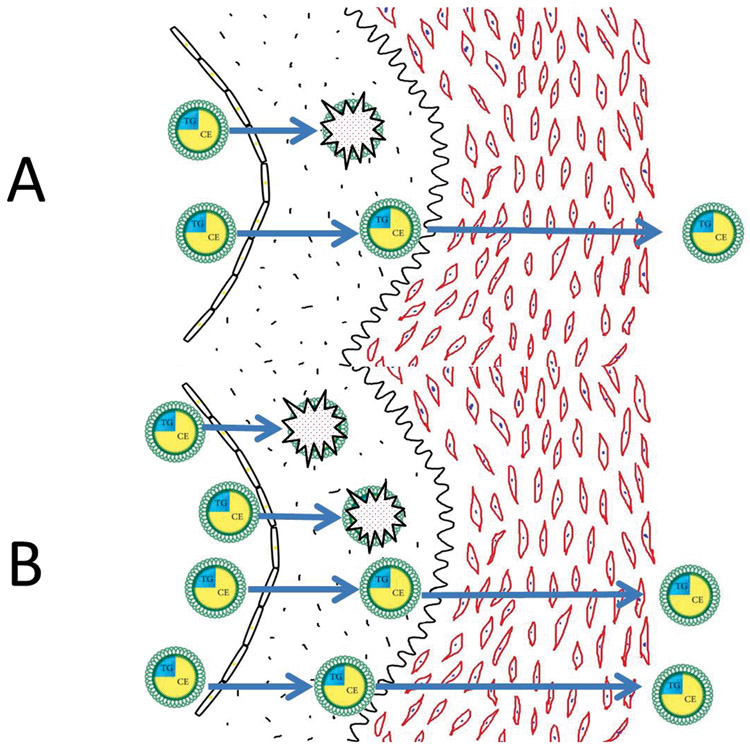
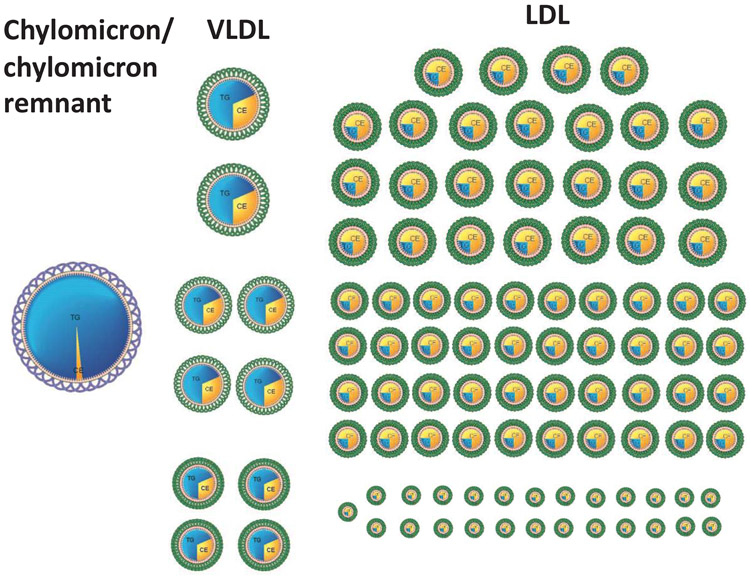
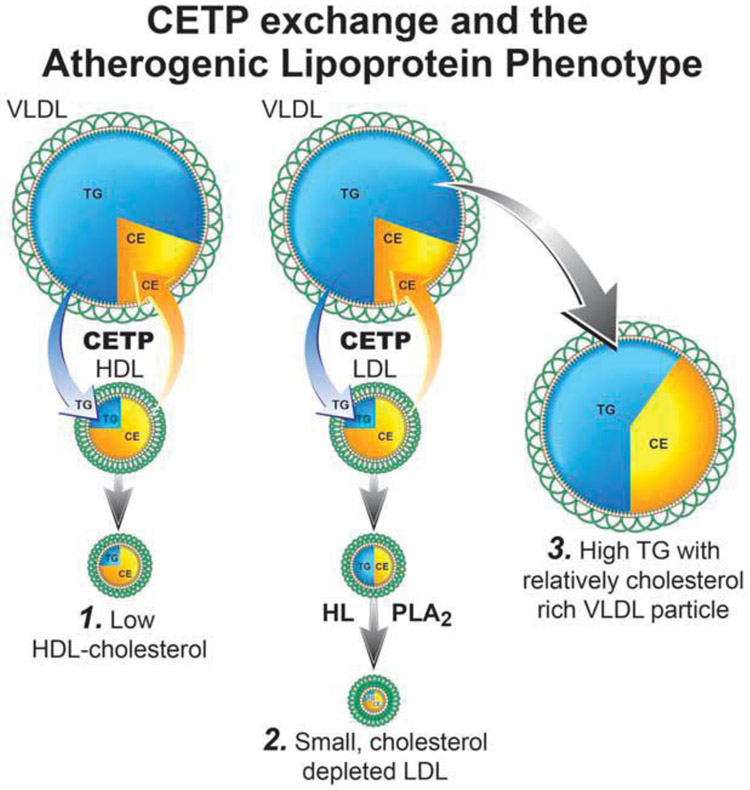
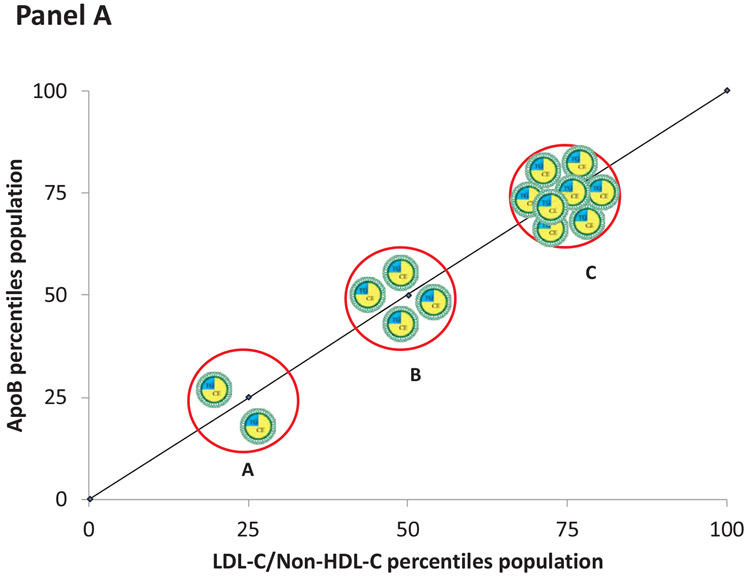
Cholesterol can only enter the arterial wall within apoB particles. However, the mass of cholesterol per apoB particle is variable. Therefore, the mass of cholesterol that will be deposited within the arterial wall is determined by the number of apoB particles that are trapped within the arterial wall. The number of apoB particles that enter the arterial wall is determined primarily by the number of apoB particles within the arterial lumen. However, once within the arterial wall, smaller cholesterol-depleted apoB particles have a greater tendency to be trapped than larger cholesterol-enriched apoB particles because they bind more avidly to the glycosaminoglycans within the subintimal space of the arterial wall. Thus, a cholesterol-enriched particle would deposit more cholesterol than a cholesterol-depleted apoB particle whereas more, smaller apoB particles that enter the arterial wall will be trapped than larger apoB particles. The net result is, with the exceptions of the abnormal chylomicron remnants in type III hyperlipoproteinemia and lipoprotein (a), all apoB particles are equally atherogenic.
Apolipoprotein B unifies, amplifies, and simplifies the information from the conventional lipid markers as to the atherogenic risk attributable to the apoB lipoproteins.
传统的动脉粥样硬化模型假定,极低密度脂蛋白颗粒、低密度脂蛋白颗粒、乳糜微粒和脂蛋白 (a) 颗粒中胆固醇的质量是决定胆固醇在动脉壁中沉积并驱动动脉粥样硬化形成的主要因素。然而,这些颗粒中的每一个都含有一个载脂蛋白 B (apoB) 分子,现在有大量证据表明,apoB 比低密度脂蛋白胆固醇或非高密度脂蛋白胆固醇更能准确地衡量载脂蛋白 B 脂蛋白的动脉粥样硬化风险。
胆固醇只能进入载脂蛋白 B 颗粒内的动脉壁。然而,每个 apoB 颗粒中的胆固醇质量是可变的。因此,沉积在动脉壁内的胆固醇质量取决于被捕获在动脉壁内的 apoB 颗粒数量。进入动脉壁的 apoB 颗粒数量主要取决于动脉腔内的 apoB 颗粒数量。然而,一旦进入动脉壁,较小的胆固醇耗竭 apoB 颗粒比较大的胆固醇富集 apoB 颗粒更有被捕获的倾向,因为它们与动脉壁内膜下空间中的糖胺聚糖结合更紧密。因此,富含胆固醇的颗粒会比胆固醇耗竭的 apoB 颗粒沉积更多的胆固醇,而进入动脉壁的更小、更小的 apoB 颗粒会比更大的 apoB 颗粒更容易被捕获。其净结果是,除了 III 型高脂蛋白血症和脂蛋白 (a) 中的异常乳糜微粒残粒外,所有 apoB 颗粒的动脉粥样硬化形成能力都相同。
载脂蛋白 B 统一、放大和简化了传统脂质标志物关于载脂蛋白 B 脂蛋白归因于动脉粥样硬化风险的信息。