Service of Oral and Maxillofacial Surgery, A Coruña University Hospital (CHUAC), Galician Health Service, A Coruña, Spain.
Department of Surgery and Medical-Surgical Specialities, School of Medicine and Dentistry, University of Santiago de Compostela, Santiago de Compostela, A Coruña, Spain.
PLoS One. 2019 Oct 25;14(10):e0224067. doi: 10.1371/journal.pone.0224067. eCollection 2019.
In early diagnosis studies on symptomatic cancer, survival was the most recommended outcome. The magnitude and impact of the patient interval and primary care interval is well-known in oral cancer; however, the hospital interval and its influence on surviving this neoplasia are not well known.
To quantify the interval between the first contact with the specialist and the start of treatment for patients with oral cancer and to evaluate whether there was a link between this interval and disease survival.
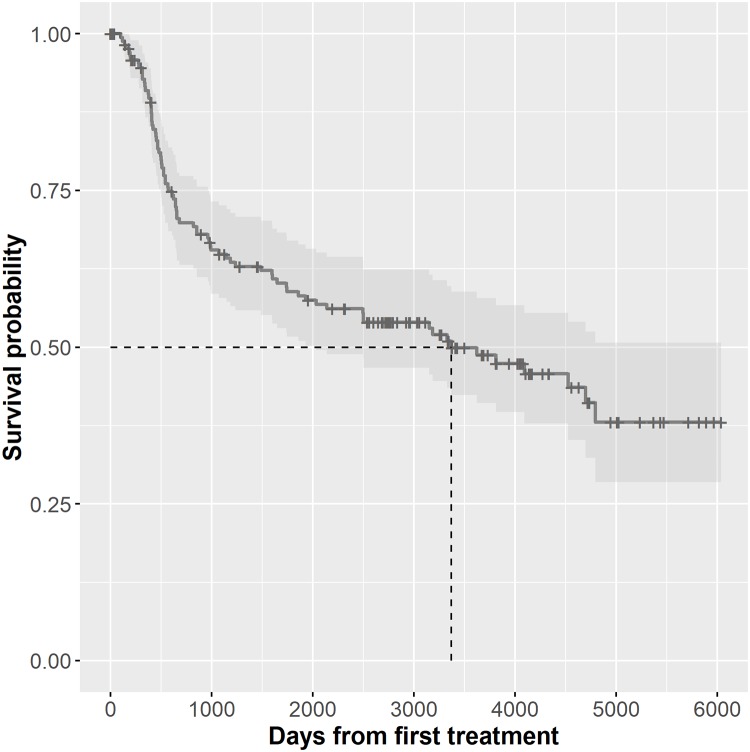
We designed a hospital-based study that included 228 patients diagnosed with oral/oropharyngeal squamous cell carcinoma between 1998 and 2008 at A Coruña University Hospital (Spain) who were followed up until 2016. The data were extracted retrospectively from hospital medical charts. The study interval was defined in the context of the "pathways to treatment" model as the interval from the first specialist visit (start point) to the start of treatment (end point). We calculated the total interval (from first symptom to treatment) to evaluate the relative length of the hospital interval, and we considered the variables age, sex, location, comorbidity and tumour classification stage. Survival time was defined as the interval from the first treatment to death or censoring.
The median hospital interval was 20 days, with an interquartile range of 15-29.1 days. The most relevant prognostic variable was the tumour stage (III-IV: Exp. ß = 2.8, p = 0.001). The hospital interval was part of the multivariate model, and its association with mortality showed a V-shaped association, where patients with short hospital intervals (3-18 days) and those with long hospital intervals (26-55 days) had significantly higher mortality than those with medium hospital intervals (19-25 days).
The hospital interval represents a relevant interval for the patient's path towards treatment, has prognostic implications and is subject to a severity bias (waiting time paradox) that should be avoided.
在有症状癌症的早期诊断研究中,生存是最常被推荐的结局。口腔癌中,患者就诊间隔和初级保健间隔的大小和影响已众所周知;然而,医院就诊间隔及其对该肿瘤生存的影响却尚未明确。
量化首诊至开始治疗的时间间隔,并评估该间隔与疾病生存之间是否存在关联。
我们设计了一项基于医院的研究,纳入了 1998 年至 2008 年期间在西班牙拉科鲁尼亚大学医院诊断为口腔/口咽鳞状细胞癌的 228 例患者,随访至 2016 年。数据从医院病历中回顾性提取。研究间隔是根据“治疗途径”模型定义的,即从首诊至开始治疗的时间间隔(起始点至终点)。我们计算了总间隔(从首症状至治疗)以评估医院间隔的相对长度,并考虑了年龄、性别、部位、合并症和肿瘤分类分期等变量。生存时间定义为从首次治疗至死亡或删失的时间间隔。
中位医院间隔为 20 天,四分位间距为 15-29.1 天。最相关的预后变量是肿瘤分期(III-IV:Exp. ß = 2.8,p = 0.001)。医院间隔是多变量模型的一部分,与死亡率的关联呈 V 形,其中 3-18 天和 26-55 天的短和长医院间隔的患者死亡率明显高于 19-25 天的患者。
医院间隔代表患者治疗途径的重要间隔,具有预后意义,并受到严重程度偏差(等待时间悖论)的影响,应避免这种偏差。