Kovatch Kevin J, Smith Joshua D, Birkeland Andrew C, Hanks John E, Jawad Rasha, McLean Scott A, Durham Alison B, Srinivasan Ashok, McHugh Jonathan B, Basura Gregory J
Department of Otolaryngology-Head and Neck Surgery, Michigan Medicine, Ann Arbor, Michigan, USA.
School of Medicine, University of Michigan, Ann Arbor, Michigan, USA.
OTO Open. 2019 Sep 13;3(3):2473974X19875077. doi: 10.1177/2473974X19875077. eCollection 2019 Jul-Sep.
To report our institutional experience, management, and outcomes of cutaneous periauricular squamous cell carcinoma (SCC).
Retrospective chart review.
Tertiary academic center.
Patients undergoing treatment of cutaneous periauricular SCC from 2000 to 2016.
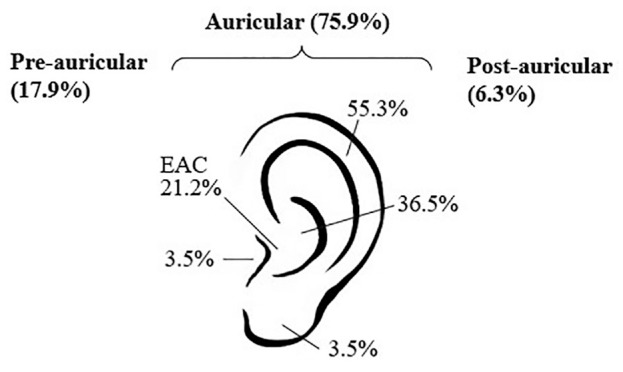
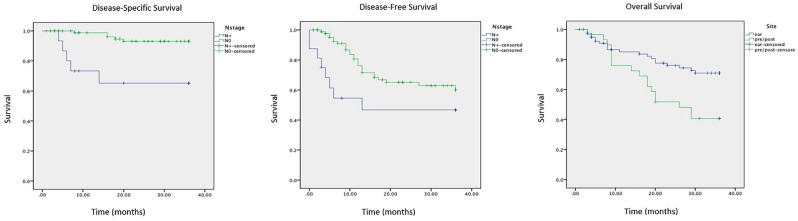
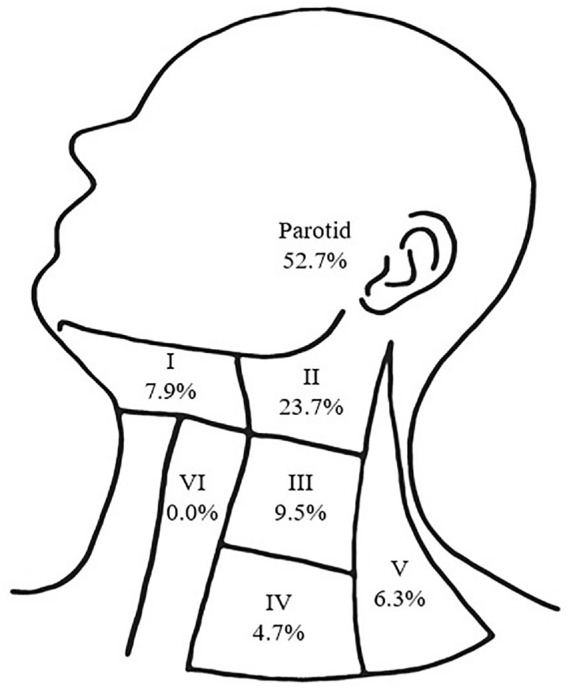
A total of 112 patients had a median follow-up of 24.5 months, a mean ± SD age of 75.7 ± 10.6 years, and a strong male predominance (93.8%). Site distribution shows 87 (77.7%) auricular, 26 (23.2%) preauricular, and 10 (8.8%) postauricular lesions. Of auricular lesions, tumors involved the tragus (n = 3, 3.4%), helix/antihelix (n = 47, 54.0%), conchal bowl (n = 31, 35.6%), external auditory canal (n = 18, 16.1%), and lobule (n = 3, 3.4%). Most patients presented at stage I (52.7%) versus stages II (28.6%), III (6.3%), and IV (12.5%). Patients were largely treated surgically with primary tumor resection ranging from wide local excision to lateral temporal bone resection (± parotidectomy and neck dissection), with 17.0% and 5.4% receiving adjuvant radiation and chemoradiation, respectively. Metastatic spread was seen to the parotid (25.9%) and neck (26.8%), with most common cervical spread to level II. Overall survival, disease-specific survival, and disease-free survival at 3 years were 62%, 89%, and 56%, respectively. Nodal disease was associated with worse disease-specific survival ( < .001) and disease-free survival ( = .042). Pre- and postauricular sites were associated with worse overall survival ( = .007) relative to auricular sites.
Among cutaneous SCC, periauricular subsites pose treatment challenges related to surrounding anatomy and represent a unique tumor population. The reported propensity toward recurrence and patterns of metastasis may better guide treatment of aggressive tumors to include regional nodal dissection.
报告我们机构对耳周皮肤鳞状细胞癌(SCC)的治疗经验、管理方法及治疗结果。
回顾性病历审查。
三级学术中心。
2000年至2016年接受耳周皮肤SCC治疗的患者。
共有112例患者,中位随访时间为24.5个月,平均年龄±标准差为75.7±10.6岁,男性占主导(93.8%)。病变部位分布显示,耳部病变87例(77.7%),耳前病变26例(23.2%),耳后病变10例(8.8%)。在耳部病变中,肿瘤累及耳屏(n = 3,3.4%)、耳轮/对耳轮(n = 47,54.0%)、耳甲腔(n = 31,35.6%)、外耳道(n = 18,16.1%)和耳垂(n = 3,3.4%)。大多数患者处于I期(52.7%),而II期(28.6%)、III期(6.3%)和IV期(12.5%)的患者较少。患者大多接受手术治疗,原发性肿瘤切除范围从广泛局部切除到颞骨外侧切除(±腮腺切除术和颈部淋巴结清扫术),分别有17.0%和5.4%的患者接受辅助放疗和放化疗。转移扩散至腮腺(25.9%)和颈部(26.8%),颈部最常见的转移部位是II区。3年总生存率、疾病特异性生存率和无病生存率分别为62%、89%和56%。淋巴结疾病与较差的疾病特异性生存率(P <.001)和无病生存率(P =.042)相关。相对于耳部病变部位,耳前和耳后病变部位的总生存率较差(P =.007)。
在皮肤SCC中,耳周亚部位因周围解剖结构而带来治疗挑战,代表了一个独特的肿瘤群体。所报告的复发倾向和转移模式可能更好地指导侵袭性肿瘤的治疗,包括区域淋巴结清扫。