Smit Cornelis, Wasmann Roeland E, Goulooze Sebastiaan C, Wiezer Marinus J, van Dongen Eric P A, Mouton Johan W, Brüggemann Roger J M, Knibbe Catherijne A J
Department of Clinical Pharmacy, St. Antonius Hospital, Nieuwegein, The Netherlands.
Department of Systems Biomedicine and Pharmacology, Leiden Academic Centre for Drug Research, Leiden University, Leiden, The Netherlands.
Br J Clin Pharmacol. 2020 Feb;86(2):303-317. doi: 10.1111/bcp.14144. Epub 2020 Jan 7.
For vancomycin treatment in obese patients, there is no consensus on the optimal dose that will lead to the pharmacodynamic target (area under the curve 400-700 mg h L ). This prospective study quantifies vancomycin pharmacokinetics in morbidly obese and nonobese individuals, in order to guide vancomycin dosing in the obese.
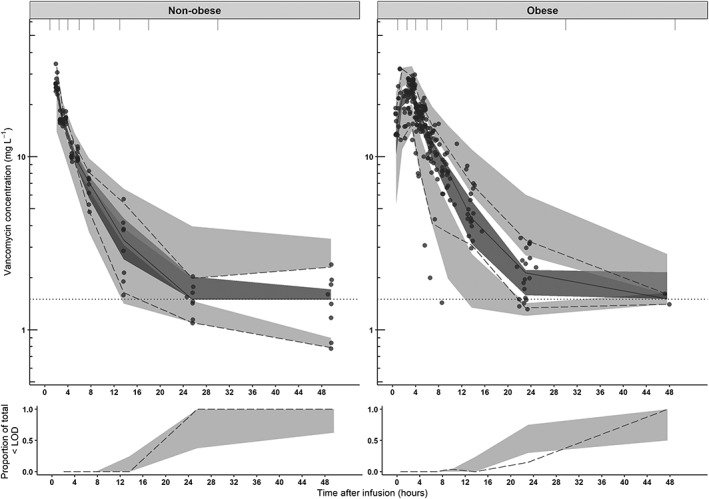
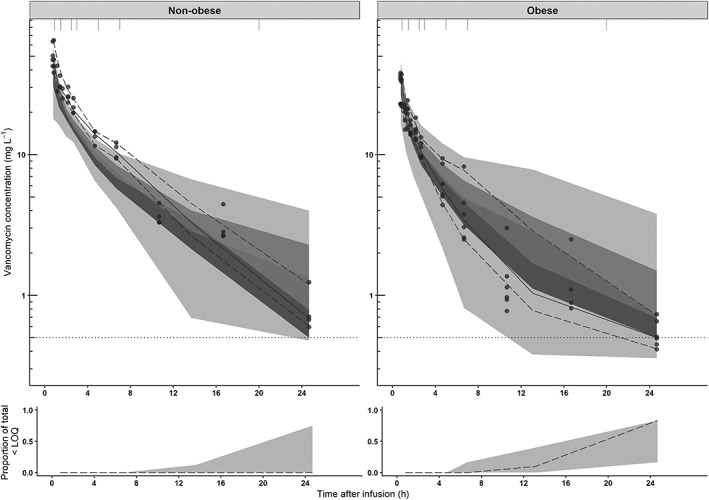
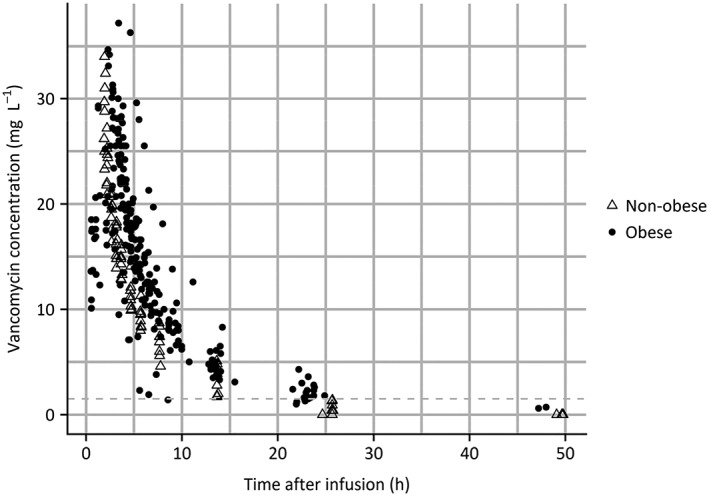
Morbidly obese individuals (n = 20) undergoing bariatric surgery and nonobese healthy volunteers (n = 8; total body weight [TBW] 60.0-234.6 kg) received a single vancomycin dose (obese: 12.5 mg kg , maximum 2500 mg; nonobese: 1000 mg) with plasma concentrations measured over 48 h (11-13 samples per individual). Modelling, internal validation, external validation using previously published data and simulations (n = 10.000 individuals, TBW 60-230 kg) were performed using NONMEM.
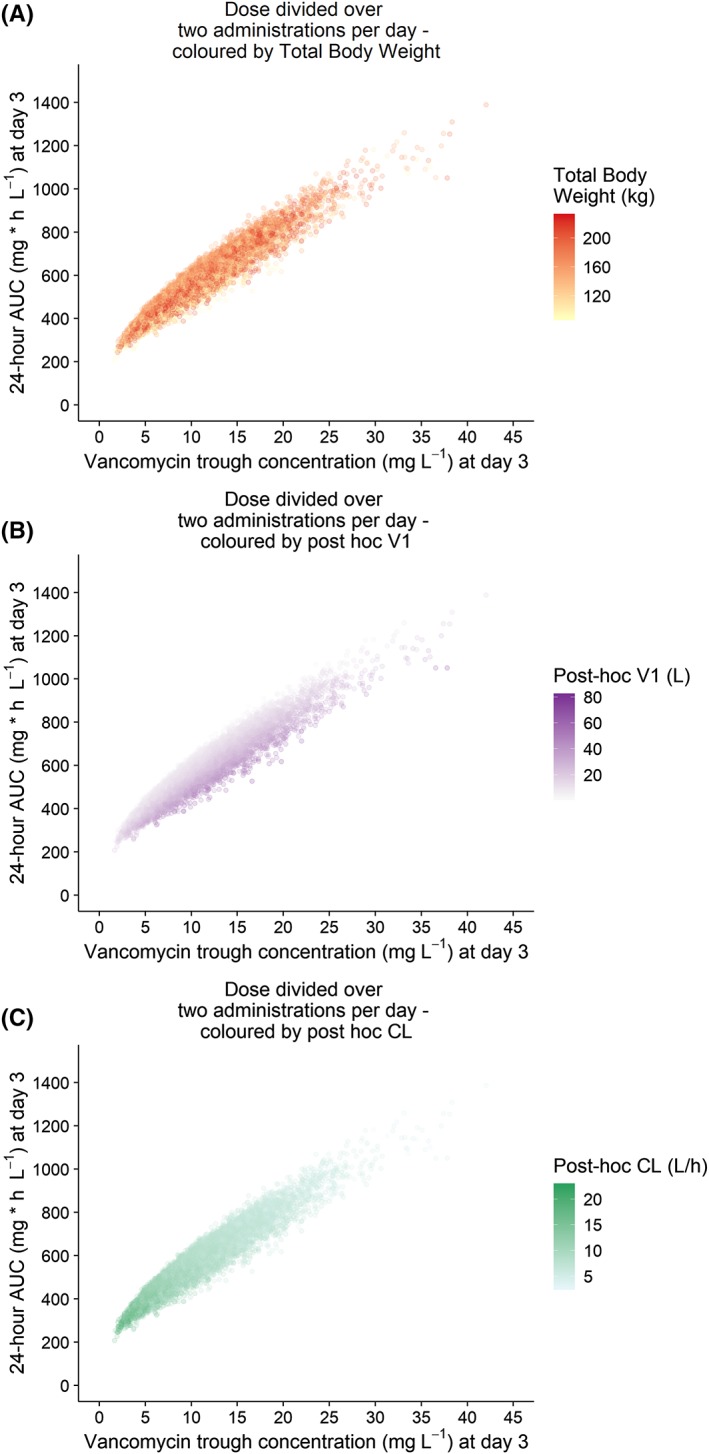
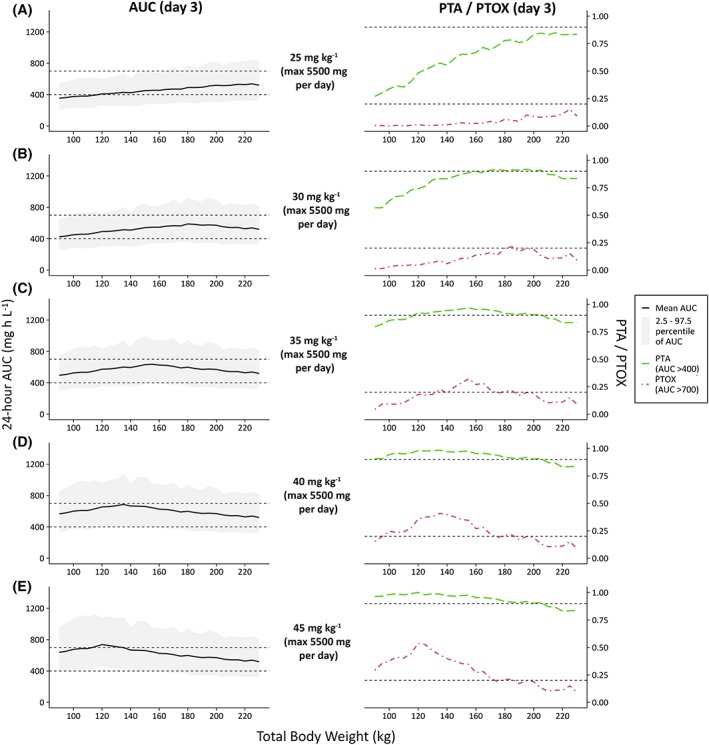
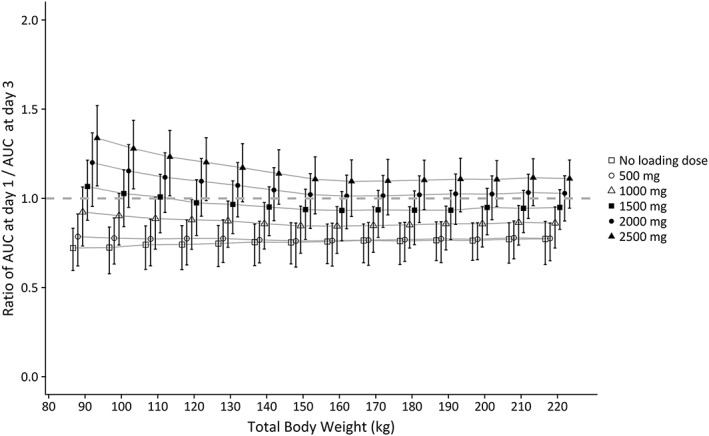
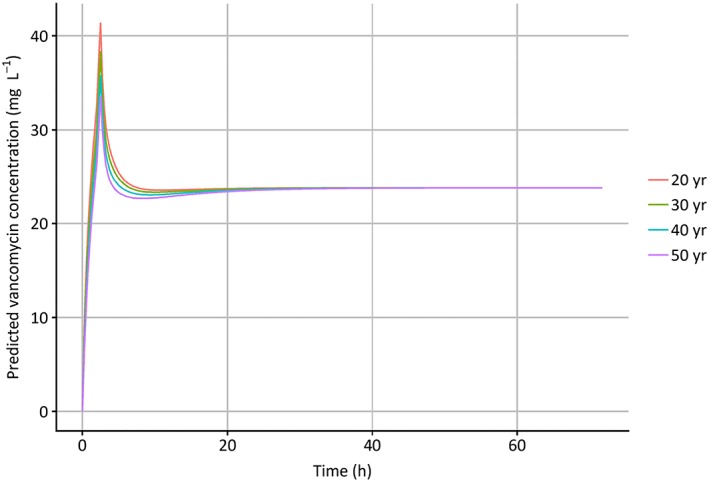
In a 3-compartment model, peripheral volume of distribution and clearance increased with TBW (both p < 0.001), which was confirmed in the external validation. A dose of 35 mg kg day (maximum 5500 mg/day) resulted in a > 90% target attainment (area under the curve > 400 mg h L ) in individuals up to 200 kg, with corresponding trough concentrations of 5.7-14.6 mg L (twice daily dosing). For continuous infusion, a loading dose of 1500 mg is required for steady state on day 1.
In this prospective, rich sampling pharmacokinetic study, vancomycin clearance was well predicted using TBW. We recommend that in obese individuals without renal impairment, vancomycin should be dosed as 35 mg kg day (maximized at 5500 mg/day). When given over 2 daily doses, trough concentrations of 5.7-14.6 mg L correspond to the target exposure in obese individuals.
对于肥胖患者的万古霉素治疗,在能达到药效学目标(曲线下面积为400 - 700mg·h/L)的最佳剂量方面尚无共识。这项前瞻性研究对病态肥胖个体和非肥胖个体的万古霉素药代动力学进行量化,以指导肥胖患者的万古霉素给药。
接受减肥手术的病态肥胖个体(n = 20)和非肥胖健康志愿者(n = 8;总体重[TBW]60.0 - 234.6kg)接受单次万古霉素剂量(肥胖者:12.5mg/kg,最大2500mg;非肥胖者:1000mg),并在48小时内测量血浆浓度(每人11 - 13个样本)。使用NONMEM进行建模、内部验证、利用先前发表的数据进行外部验证以及模拟(n = 10000个体,TBW 60 - 230kg)。
在三室模型中,外周分布容积和清除率随总体重增加而增加(两者p < 0.001),这在外部验证中得到证实。对于体重达200kg的个体,剂量为35mg/kg·天(最大5500mg/天)可使>90%的患者达到目标(曲线下面积>400mg·h/L),相应的谷浓度为5.7 - 14.6mg/L(每日两次给药)。对于持续输注,第1天达到稳态需要1500mg的负荷剂量。
在这项前瞻性、采样丰富的药代动力学研究中,使用总体重能很好地预测万古霉素清除率。我们建议,在无肾功能损害的肥胖个体中,万古霉素的给药剂量应为35mg/kg·天(最大5500mg/天)。每日分两次给药时,谷浓度为5.7 - 14.6mg/L符合肥胖个体的目标暴露量。