Department of Medicine, VU University Medical Centre Amsterdam, Amsterdam, the Netherlands.
Department of Medicine, Montreal Heart Institute, Université de Montréal, Montreal, Canada.
BMC Med. 2019 Nov 1;17(1):197. doi: 10.1186/s12916-019-1433-3.
Dyslipidemia and inflammation are closely interrelated contributors in the pathogenesis of atherosclerosis. Disorders of lipid metabolism initiate an inflammatory and immune-mediated response in atherosclerosis, while low-density lipoprotein cholesterol (LDL-C) lowering has possible pleiotropic anti-inflammatory effects that extend beyond lipid lowering.
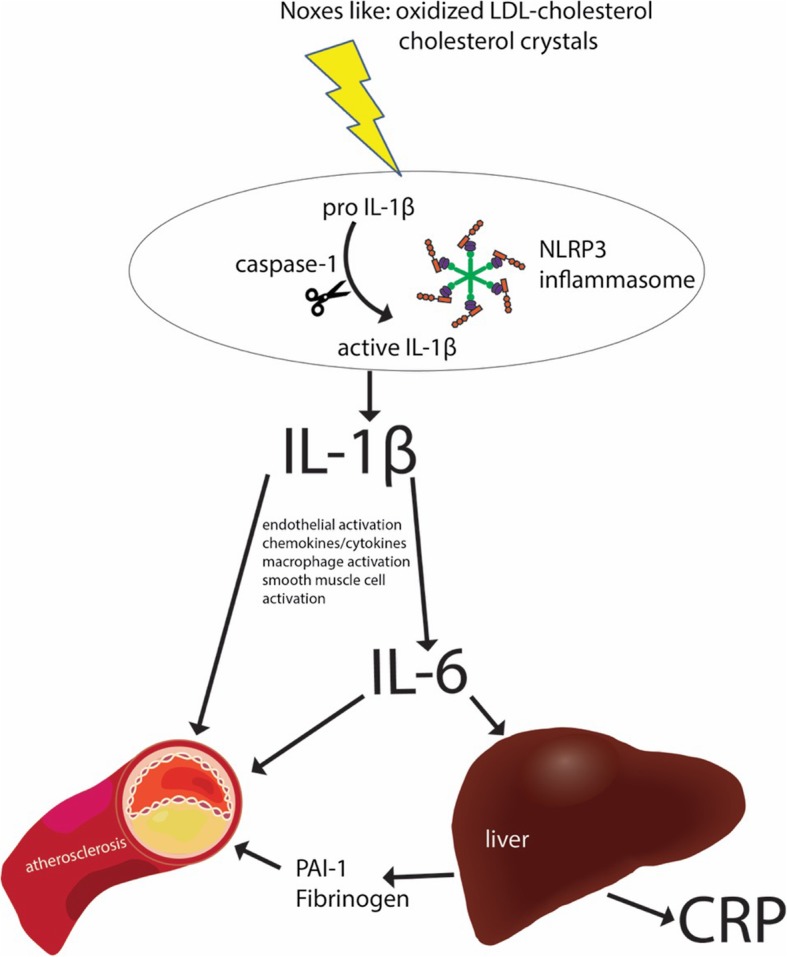
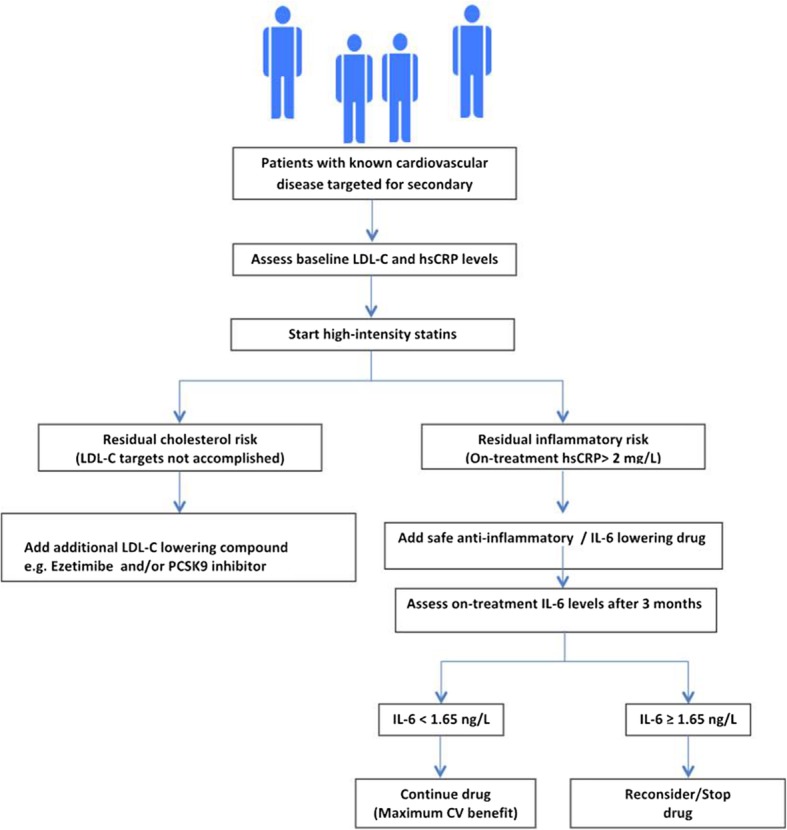
Activation of the immune system/inflammasome destabilizes the plaque, which makes it vulnerable to rupture, resulting in major adverse cardiac events (MACE). The activated immune system potentially accelerates atherosclerosis, and atherosclerosis activates the immune system, creating a vicious circle. LDL-C enhances inflammation, which can be measured through multiple parameters like high-sensitivity C-reactive protein (hsCRP). However, multiple studies have shown that CRP is a marker of residual risk and not, itself, a causal factor. Recently, anti-inflammatory therapy has been shown to decelerate atherosclerosis, resulting in fewer MACE. Nevertheless, an important side effect of anti-inflammatory therapy is the potential for increased infection risk, stressing the importance of only targeting patients with high residual inflammatory risk. Multiple (auto-)inflammatory diseases are potentially related to/influenced by LDL-C through inflammasome activation.
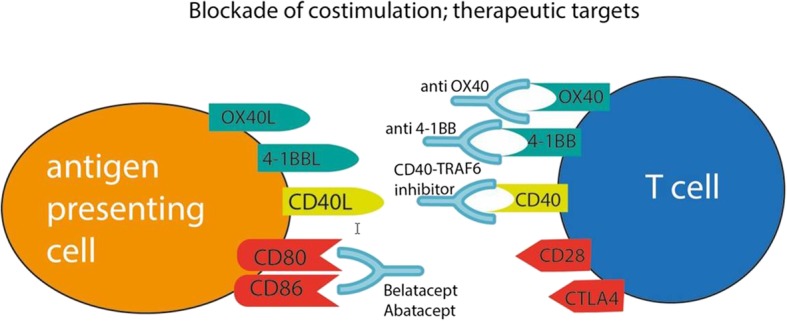
Research suggests that LDL-C induces inflammation; inflammation is of proven importance in atherosclerotic disease progression; anti-inflammatory therapies yield promise in lowering (cardiovascular) disease risk, especially in selected patients with high (remaining) inflammatory risk; and intriguing new anti-inflammatory developments, for example, in nucleotide-binding leucine-rich repeat-containing pyrine receptor inflammasome targeting, are currently underway, including novel pathway interventions such as immune cell targeting and epigenetic interference. Long-term safety should be carefully monitored for these new strategies and cost-effectiveness carefully evaluated.
血脂异常和炎症是动脉粥样硬化发病机制中密切相关的两个因素。脂质代谢紊乱在动脉粥样硬化中引发炎症和免疫介导反应,而降低低密度脂蛋白胆固醇(LDL-C)可能具有除降低脂质以外的多效抗炎作用。
免疫系统/炎症小体的激活使斑块不稳定,从而使其易于破裂,导致主要不良心脏事件(MACE)。激活的免疫系统可能会加速动脉粥样硬化,而动脉粥样硬化会激活免疫系统,形成一个恶性循环。LDL-C 增强炎症,这可以通过多个参数来衡量,如高敏 C 反应蛋白(hsCRP)。然而,多项研究表明 CRP 是残余风险的标志物,而不是其本身就是一个因果因素。最近,抗炎治疗已被证明可以减缓动脉粥样硬化的发展,从而减少 MACE 的发生。然而,抗炎治疗的一个重要副作用是增加感染风险的可能性,这强调了仅针对高残余炎症风险患者进行靶向治疗的重要性。多种(自身)炎症性疾病可能通过炎症小体激活与 LDL-C 有关/受其影响。
研究表明,LDL-C 可诱导炎症;炎症在动脉粥样硬化疾病进展中具有重要作用;抗炎治疗有望降低(心血管)疾病风险,尤其是在具有高(剩余)炎症风险的选定患者中;目前正在进行有趣的新抗炎发展,例如核苷酸结合富含亮氨酸重复序列的受体炎性小体靶向治疗,包括免疫细胞靶向和表观遗传干扰等新的途径干预。应仔细监测这些新策略的长期安全性,并对其成本效益进行仔细评估。