Eade Thomas, Hruby George, Booth Jeremy, Bromley Regina, Guo Lesley, O'Toole Andrew, Le Andrew, Wu Kenny, Whitaker May, Rasiah Krishan, Chalasani Venu, Vass Justin, Kwong Carolyn, Atyeo John, Kneebone Andrew
Department of Radiation Oncology Royal North Shore Hospital, St. Leonards, New South Wales, Australia.
Sydney Medical School, University of Sydney, Sydney, Australia.
Adv Radiat Oncol. 2019 Apr 11;4(4):623-630. doi: 10.1016/j.adro.2019.03.015. eCollection 2019 Oct-Dec.
To demonstrate feasibility and toxicity of linear accelerator-based stereotactic radiation therapy boost (SBRT) for prostate cancer, mimicking a high-dose-rate brachytherapy boost.
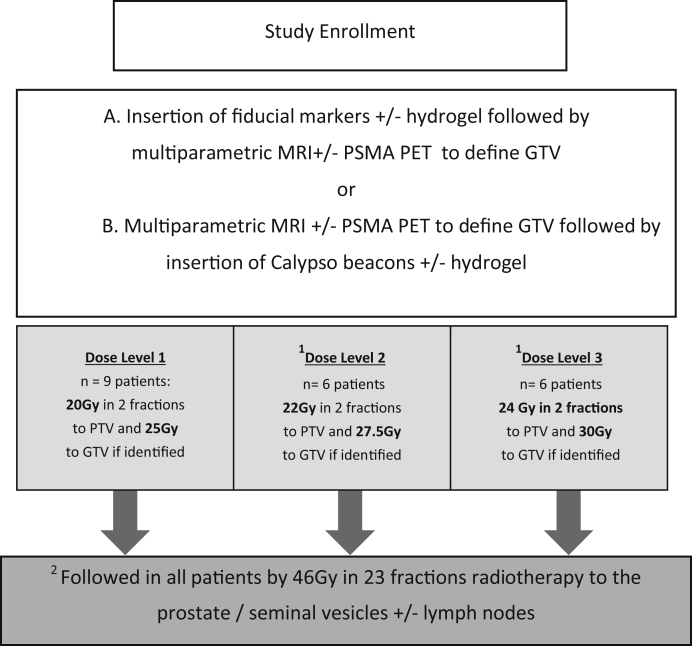
A phase 1 sequential dose escalation study of SBRT compared 20 Gy, 22 Gy, and 24 Gy to the prostate and 25 Gy, 27.5 Gy, and 30 Gy to the gross tumor volume in 2 fractions, combined with 46 Gy in 23 fractions of external beam radiation. Feasibility of dose escalation (volume receiving 125% and 150% of the dose) while meeting organ-at-risk dose constraints, grade 2 acute and late gastrointestinal and genitourinary toxicity, and freedom from biochemical failure were secondary endpoints.
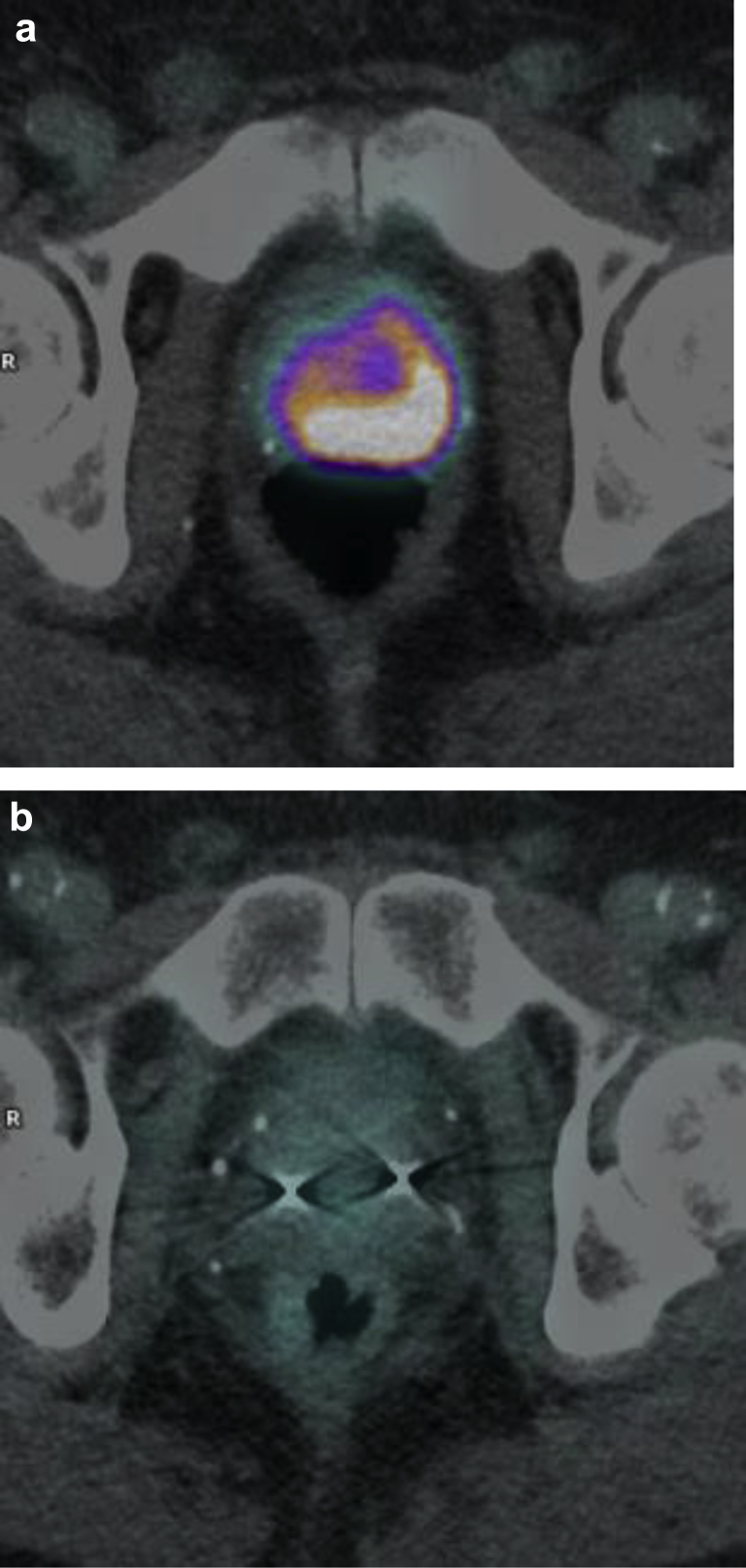
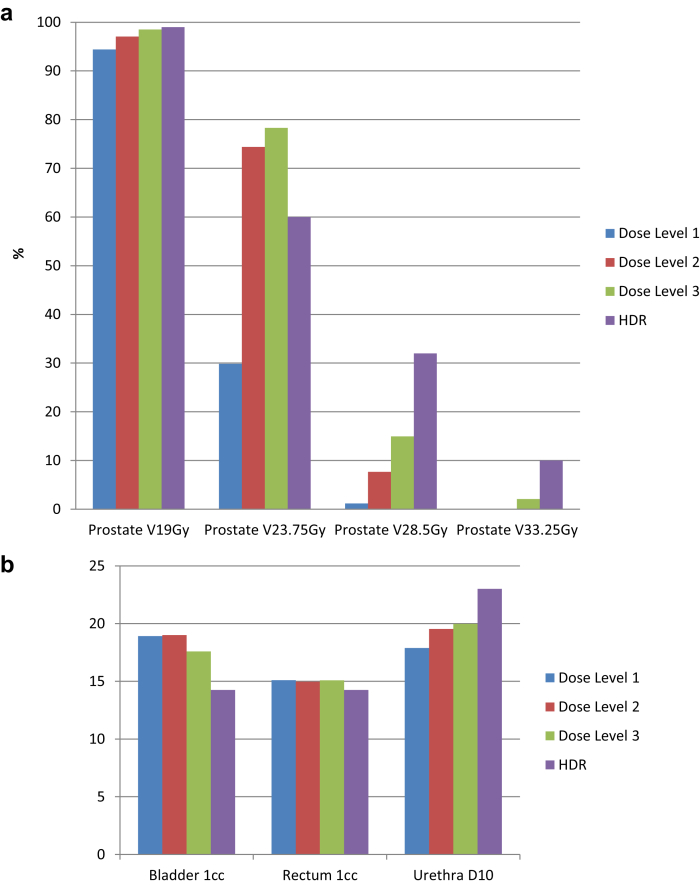
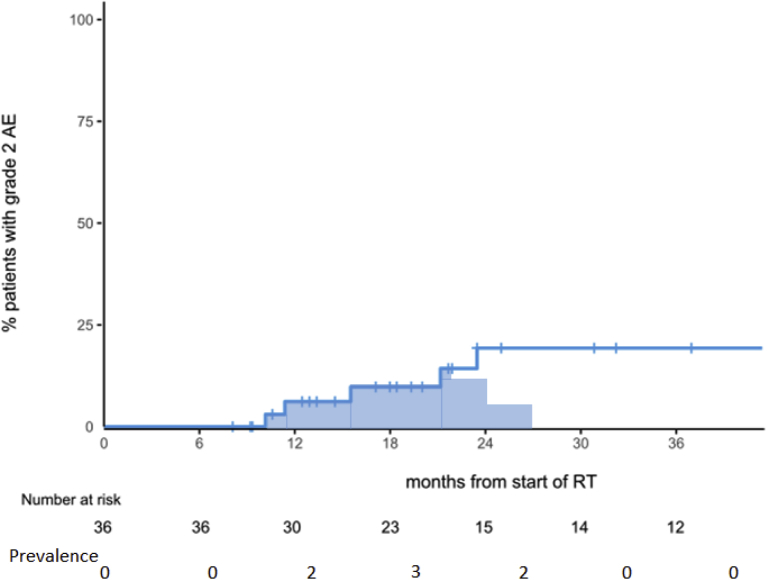
Thirty-six men with intermediate- and high-risk prostate cancer were enrolled with a median follow-up of 24 months. Sixty-four percent of patients had high-risk features. Nine men were enrolled to dose level 1, 6 to level 2, and 6 to level 3. Another 15 patients were treated at dose level 3 on the continuation study. Dose level 3 achieved superior 125% (23.75 Gy) and 150% (28.5 Gy) dose compared to dose levels 1 and 2, with minimal differences in organ-at-risk doses. Kaplan-Meier estimate of freedom from biochemical failure at 3 years was 93.3%. There were no late grade 2 or 3 gastrointestinal events. The late grade 2 genitourinary toxicity at 2 years was 19.3%. Prostate-specific membrane antigen positron emission tomography was performed at 2 years with no local recurrences.
We have shown that a linear accelerator-based SBRT boost for prostate cancer is feasible and can achieve doses comparable to high-dose-rate boost up to the 150% isodose volumes. Rectal, bladder, and urethral doses remained low, and long-term toxicity was the same as or better than previous reports from high-dose-rate or low-dose-rate boost protocols.
证明基于直线加速器的立体定向放射治疗增敏(SBRT)用于前列腺癌的可行性和毒性,模拟高剂量率近距离放射治疗增敏。
一项SBRT的1期序贯剂量递增研究比较了20Gy、22Gy和24Gy给予前列腺,以及25Gy、27.5Gy和30Gy给予大体肿瘤体积,分2次给予,联合外照射46Gy分23次给予。在满足危及器官剂量限制的同时剂量递增(接受125%和150%剂量的体积)的可行性、2级急性和晚期胃肠道及泌尿生殖系统毒性以及无生化失败是次要终点。
36例中高危前列腺癌男性入组,中位随访24个月。64%的患者具有高危特征。9例男性入组剂量水平1,6例入组剂量水平2,6例入组剂量水平3。另外15例患者在延续研究中接受剂量水平3的治疗。与剂量水平1和2相比,剂量水平3实现了更高的125%(23.75Gy)和150%(28.5Gy)剂量,危及器官剂量差异最小。3年时无生化失败的Kaplan-Meier估计值为93.3%。无晚期2级或3级胃肠道事件。2年时晚期2级泌尿生殖系统毒性为19.3%。2年时进行前列腺特异性膜抗原正电子发射断层扫描,无局部复发。
我们已经表明,基于直线加速器的SBRT用于前列腺癌增敏是可行的,并且可以达到与高剂量率增敏相当的剂量,直至150%等剂量体积。直肠、膀胱和尿道剂量保持较低,长期毒性与高剂量率或低剂量率增敏方案的既往报告相同或更好。