Department of Clinical Epidemiology and Data Science, Department of Obstetrics & Gynecology, Amsterdam Public Health Research Institute, Amsterdam UMC, Location Academic Medical Center, University of Amsterdam, Amsterdam, The Netherlands.
GROW - School for Oncology and Developmental Biology, Maastricht and Department of Obstetrics and Gynecology Máxima Medical Centre Veldhoven, The Netherlands.
Ultrasound Obstet Gynecol. 2021 Apr;57(4):582-591. doi: 10.1002/uog.21907.
To evaluate whether there is a differential benefit of planned Cesarean delivery (CD) over planned vaginal delivery (VD) in women with a twin pregnancy and the first twin in cephalic presentation, depending on prespecified baseline maternal and pregnancy characteristics, and/or gestational age (GA) at delivery.
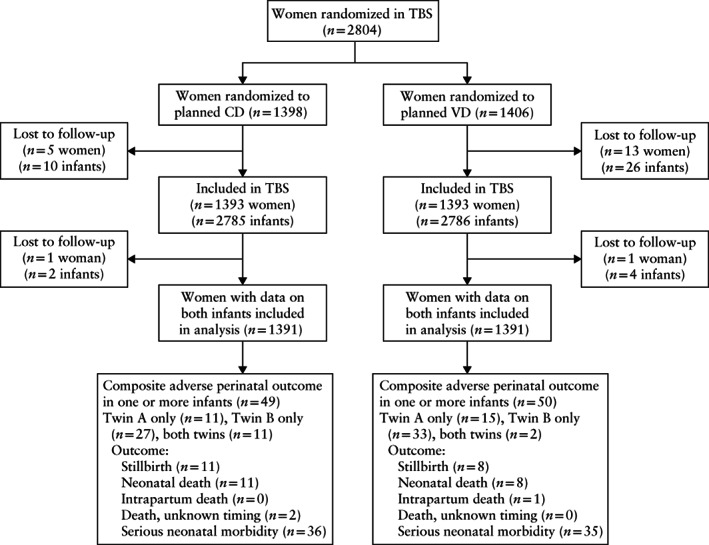
This was a secondary analysis of the Twin Birth Study, which included 2804 women with a twin pregnancy and the first twin (Twin A) in cephalic presentation between 32 + 0 and 38 + 6 weeks' gestation at 106 centers in 25 countries. Women were assigned randomly to either planned CD or planned VD. The main outcome measure was composite adverse perinatal outcome, defined as the occurrence of perinatal mortality or serious neonatal morbidity in at least one twin. The baseline maternal and pregnancy characteristics (markers) considered were maternal age, parity, history of CD, use of antenatal corticosteroids, estimated fetal weight (EFW) of Twin A, EFW of Twin B, > 25% difference in EFW between the twins, presentation of Twin B, chorionicity on ultrasound, method of conception, complications of pregnancy, ruptured membranes at randomization and GA at randomization. Separate logistic regression models were developed for each marker in order to model composite adverse perinatal outcome as a function of the specific marker, planned delivery mode and the interaction between these two terms. In addition, multivariable logistic regression analysis with backward variable elimination was performed separately in each arm of the trial. The association between planned mode of delivery and composite adverse perinatal outcome, according to GA at delivery, was assessed using logistic regression analysis.
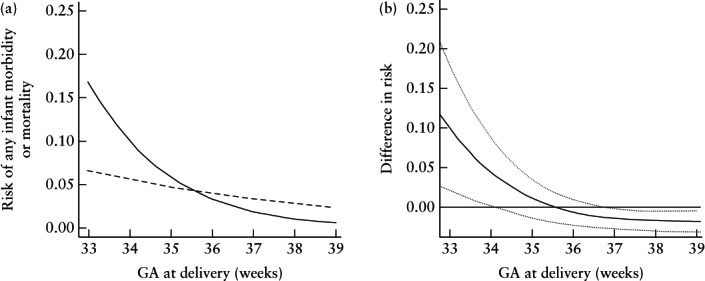
Of the 2804 women initially randomized, 1391 were included in each study arm. None of the studied baseline markers was associated with a differential benefit of planned CD over planned VD in the rate of composite adverse perinatal outcome. GA at delivery was associated differentially with composite adverse perinatal outcome in the treatment arms (P for interaction < 0.001). Among pregnancies delivered at 32 + 0 to 36 + 6 weeks, there was a trend towards a lower rate of composite adverse perinatal outcome in those in the planned-VD group compared with those in planned-CD group (29 (2.2%) vs 48 (3.6%) cases; odds ratio (OR) 0.62 (95% CI, 0.37-1.03)). In pregnancies delivered at or after 37 + 0 weeks, planned VD was associated with a significantly higher rate of composite adverse perinatal outcome, as compared with planned CD (23 (1.5%) vs 10 (0.7%) cases; OR, 2.25 (95% CI, 1.06-4.77)).
The perinatal outcome of twin pregnancies with the first twin in cephalic presentation may differ depending on GA at delivery and planned mode of delivery. At 32-37 weeks, planned VD seems to be favorable, while, from around 37 weeks onwards, planned CD might be safer. The absolute risks of adverse perinatal outcomes at term are low and must be weighed against the increased maternal risks associated with planned CD. © 2019 The Authors. Ultrasound in Obstetrics & Gynecology published by John Wiley & Sons Ltd on behalf of International Society of Ultrasound in Obstetrics and Gynecology.
评估对于头位双胎妊娠且第一胎儿为头位的产妇,是否存在计划性剖宫产优于计划性阴道分娩的差异获益,具体取决于特定的基线产妇和妊娠特征以及/或分娩时的孕龄(GA)。
这是对 Twin Birth 研究的二次分析,该研究纳入了 2804 例孕 32+0 至 38+6 周且头位的双胎妊娠产妇,其中第一胎儿(Twin A)位于头位,共 106 个中心来自 25 个国家。产妇被随机分配至计划性剖宫产或计划性阴道分娩组。主要结局指标为复合围产儿不良结局,定义为至少有一胎发生围产儿死亡或严重新生儿并发症。考虑的基线产妇和妊娠特征(标志物)包括产妇年龄、产次、剖宫产史、产前使用皮质类固醇、Twin A 的估计胎儿体重(EFW)、Twin B 的 EFW、双胞胎之间 EFW 差值>25%、Twin B 的先露部位、超声检查的绒毛膜性、受孕方式、妊娠并发症、随机分组时胎膜破裂以及随机分组时的 GA。针对每个标志物分别建立了单独的逻辑回归模型,以将复合围产儿不良结局作为特定标志物、计划分娩方式以及这两个因素之间的交互作用的函数进行建模。此外,在每个试验组中分别进行了多变量逻辑回归分析和逐步变量消除。使用逻辑回归分析评估根据分娩时 GA 计划分娩方式与复合围产儿不良结局之间的关联。
在最初随机分组的 2804 例产妇中,1391 例被纳入每个研究组。在研究中没有一个基线标志物与计划性剖宫产与计划性阴道分娩的复合围产儿不良结局率之间的差异获益相关。分娩时的 GA 与治疗组中的复合围产儿不良结局具有显著的相关性(P < 0.001)。在 32+0 至 36+6 周分娩的妊娠中,计划性阴道分娩组的复合围产儿不良结局率有降低的趋势,而计划性剖宫产组则较高(29 例(2.2%)vs 48 例(3.6%);比值比(OR)0.62(95%CI,0.37-1.03))。在 37+0 周及以上分娩的妊娠中,与计划性剖宫产相比,计划性阴道分娩与复合围产儿不良结局的发生率显著升高(23 例(1.5%)vs 10 例(0.7%);OR,2.25(95%CI,1.06-4.77))。
头位双胎妊娠第一胎儿的围产儿结局可能取决于分娩时的 GA 和计划分娩方式。在 32-37 周时,计划性阴道分娩似乎是有利的,而在大约 37 周以后,计划性剖宫产可能更安全。足月时不良围产儿结局的绝对风险较低,必须权衡与计划性剖宫产相关的增加的产妇风险。© 2019 作者。超声在妇产科由约翰威立父子有限公司代表国际妇产科超声学会出版。