University of the Western Cape, Cape Town, South Africa.
Medical Rehabilitation College, Box 256, Blantyre, Malawi.
BMC Health Serv Res. 2019 Nov 4;19(1):789. doi: 10.1186/s12913-019-4654-4.
Stroke is a major public health concern, affecting millions of people worldwide. Care of the condition however, remain inconsistent in developing countries. The purpose of this scoping review was to document evidence of stroke care and service delivery in low and middle-income countries to better inform development of a context-fit stroke model of care.
An interpretative scoping literature review based on Arksey and O'Malley's five-stage-process was executed. The following databases searched for literature published between 2010 and 2017; Cochrane Library, Credo Reference, Health Source: Nursing/Academic Edition, Science Direct, BioMed Central, Cumulative Index to Nursing and Allied Health Literature (CINNAHL), Academic Search Complete, and Google Scholar. Single combined search terms included acute stroke, stroke care, stroke rehabilitation, developing countries, low and middle-income countries.
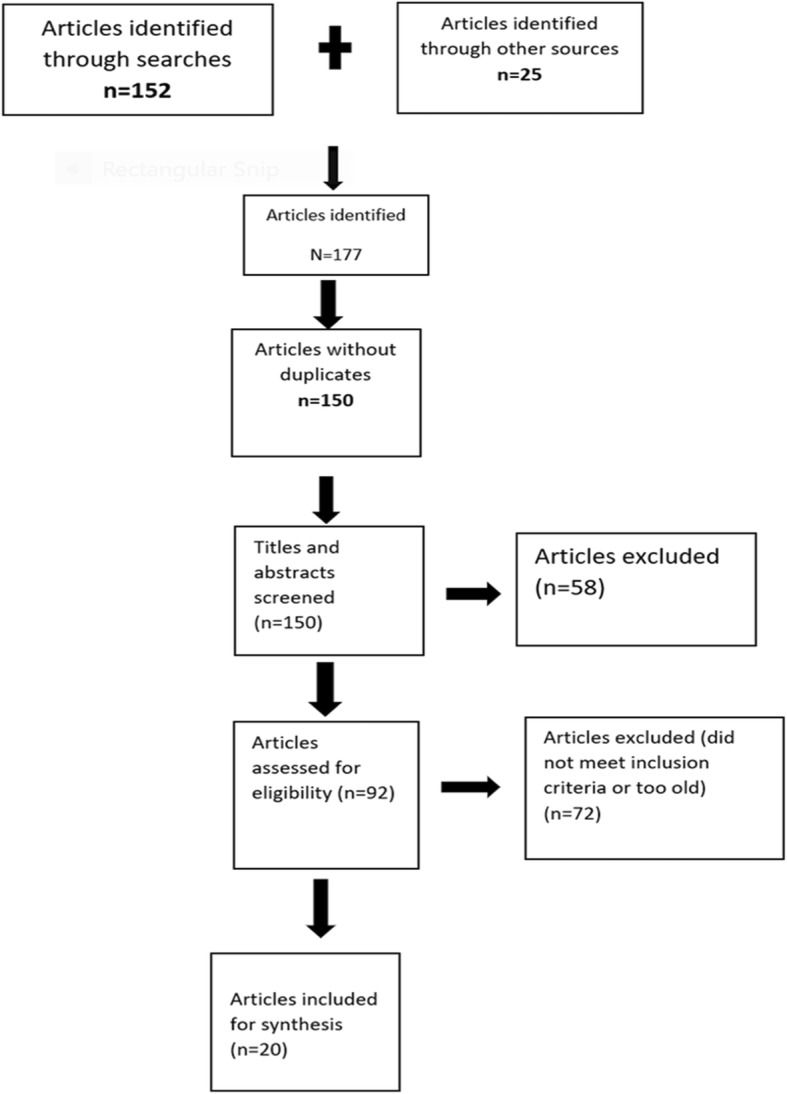
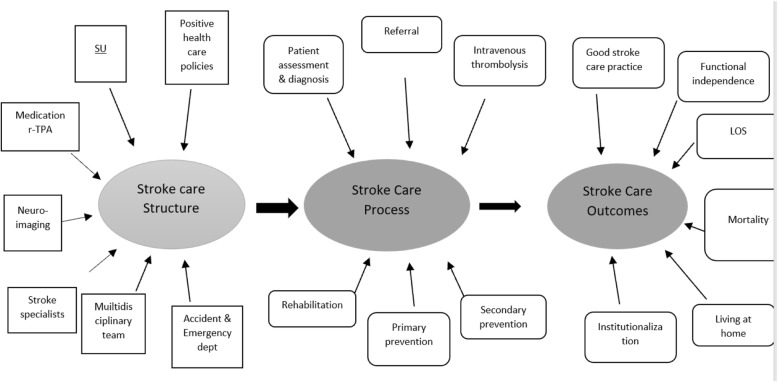
A total of 177 references were identified. Twenty of them, published between 2010 and 2017, were included in the review. Applying the Donebedian Model of quality of care, seven dimensions of stroke-care structure, six dimensions of stroke care processes, and six dimensions of stroke care outcomes were identified. Structure of stroke care included availability of a stroke unit, an accident and emergency department, a multidisciplinary team, stroke specialists, neuroimaging, medication, and health care policies. Stroke care processes that emerged were assessment and diagnosis, referrals, intravenous thrombolysis, rehabilitation, and primary and secondary prevention strategies. Stroke-care outcomes included quality of stroke-care practice, functional independence level, length of stay, mortality, living at home, and institutionalization.
There is lack of uniformity in the way stroke care is advanced in low and middle-income countries. This is reflected in the unsatisfactory stroke care structure, processes, and outcomes. There is a need for stroke care settings to adopt quality improvement strategies. Health ministry and governments need to decisively face stroke burden by setting policies that advance improved care of patients with stroke. Stroke Units and Recombinant Tissue Plasminogen Activator (rtPA) administration could be considered as both a structural and process necessity towards improvement of outcomes of patients with stroke in the LMICs.
中风是一个重大的公共卫生问题,影响着全世界数百万人。然而,在发展中国家,中风的护理仍然不一致。本范围综述的目的是记录中风护理和服务提供在低收入和中等收入国家的证据,以便更好地为制定适合国情的中风护理模式提供信息。
根据 Arksey 和 O'Malley 的五阶段过程,进行了解释性范围综述。在 2010 年至 2017 年期间,在以下数据库中搜索文献:Cochrane 图书馆、Credo Reference、Health Source: Nursing/Academic Edition、Science Direct、BioMed Central、Cumulative Index to Nursing and Allied Health Literature (CINNAHL)、Academic Search Complete 和 Google Scholar。单一的综合搜索词包括急性中风、中风护理、中风康复、发展中国家、低收入和中等收入国家。
共确定了 177 篇参考文献。其中 20 篇发表于 2010 年至 2017 年,纳入了本次综述。应用 Donebedian 护理质量模型,确定了中风护理结构的七个维度、中风护理过程的六个维度和中风护理结果的六个维度。中风护理结构包括中风单元、急诊室、多学科团队、中风专家、神经影像学、药物和医疗保健政策的可用性。出现的中风护理过程包括评估和诊断、转介、静脉内溶栓、康复以及初级和二级预防策略。中风护理结果包括中风护理实践的质量、功能独立性水平、住院时间、死亡率、居家生活和机构化。
中风在低收入和中等收入国家的护理方式缺乏一致性。这反映在中风护理结构、过程和结果的不满意上。中风护理环境需要采取质量改进策略。卫生部和政府需要通过制定推进中风患者护理的政策,果断地应对中风负担。中风单元和重组组织型纤溶酶原激活剂(rtPA)的使用可以被认为是改善中低收入国家中风患者结局的结构和过程的必要条件。