Department of Hepatobiliary Surgery, the First Affiliated Hospital of Guangzhou University of Chinese Medicine, 16 Airport Road, Guangzhou, 510405, China.
Lingnan Medical Research Center, Guangzhou University of Chinese Medicine, Guangzhou, 510405, China.
BMC Cancer. 2019 Nov 6;19(1):1047. doi: 10.1186/s12885-019-6240-x.
The application of laparoscopic liver resection (LLR) has expanded rapidly in recent decades. Although multiple authors have reported LLR shows improved safety and efficacy in treating hepatocellular carcinoma (HCC) compared with open liver resection (OLR), laparoscopic (LMLR) and open (OMLR) major liver resections for HCC treatment remain inadequately evaluated. This work aimed to test the hypothesis that LMLR is safer and more effective than OMLR for HCC.
Comparative cohort and registry studies on LMLR and OMLR, searched in PubMed, the Science Citation Index, EMBASE, and the Cochrane Library, and published before March 31, 2018, were collected systematically and meta-analyzed. Fixed- and random-effects models were employed for generating pooled estimates. Heterogeneity was assessed by the Q-statistic.
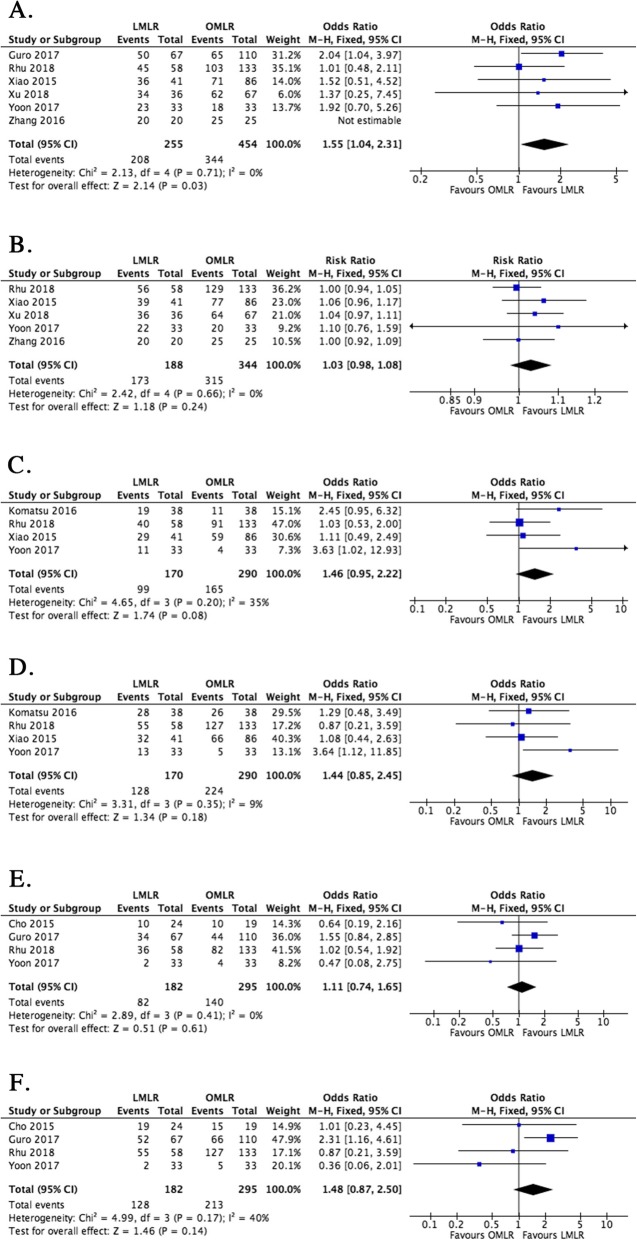
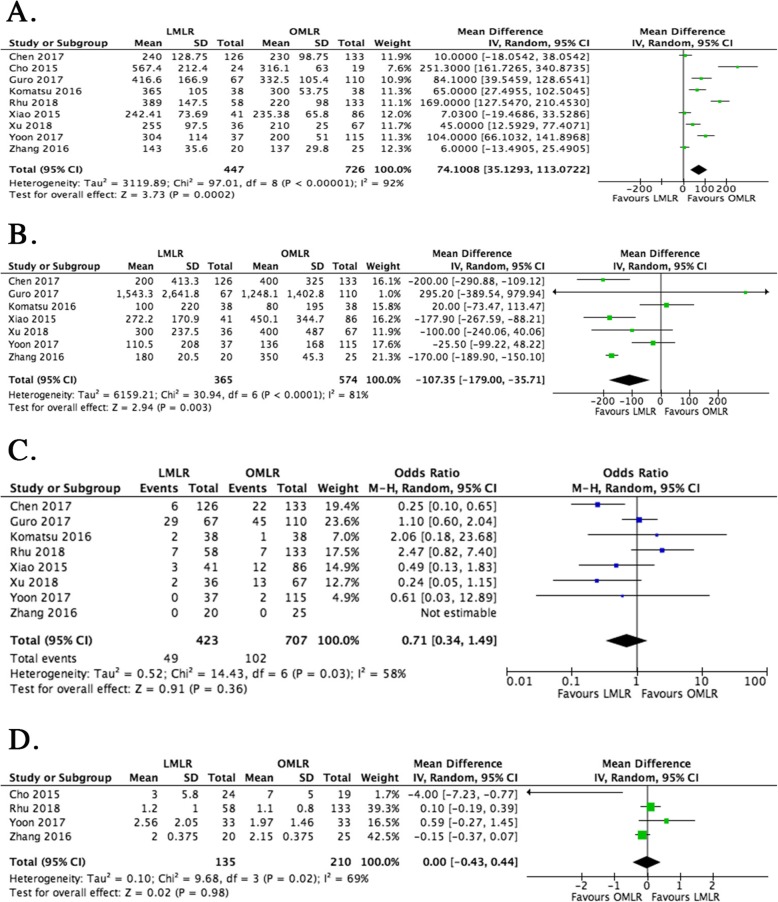
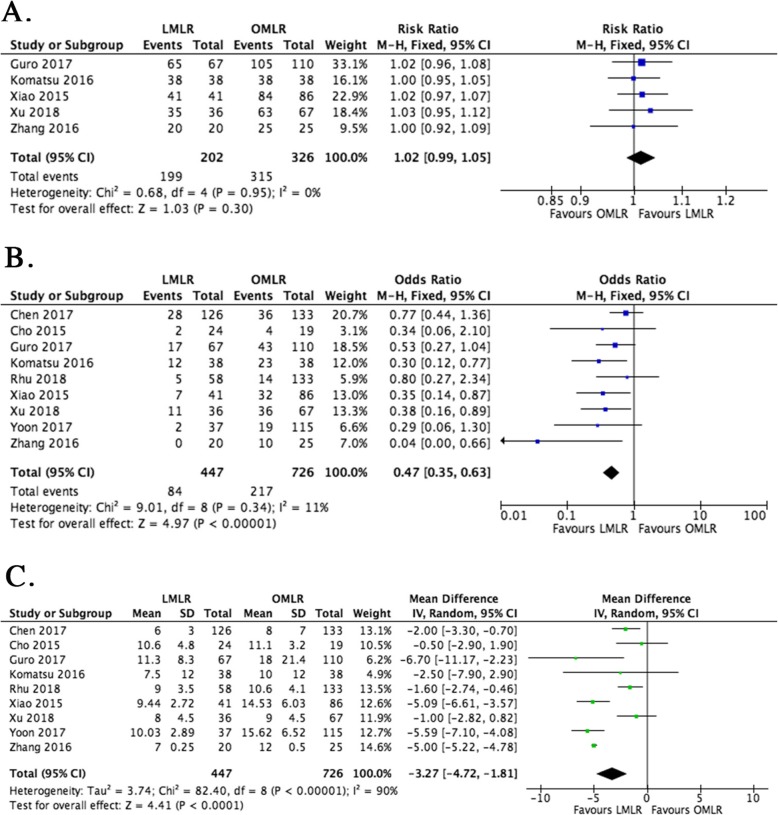
Nine studies (1173 patients) were included. Although the pooled data showed operation time was markedly increased for LMLR in comparison with OMLR (weighted mean difference [WMD] 74.1, 95% CI 35.1 to 113.1, P = 0.0002), blood loss was reduced (WMD = - 107.4, 95% CI - 179.0 to - 35.7, P = 0.003), postoperative morbidity was lower (odds ratio [OR] 0.47, 95% CI 0.35 to 0.63, P < 0.0001), and hospital stay was shorter (WMD = - 3.27, 95% CI - 4.72 to - 1.81, P < 0.0001) in the LMLR group. Although 1-year disease-free survival (DFS) was increased in patients administered LMLR (OR = 1.55, 95% CI 1.04 to 2.31, P = 0.03), other 1-, 3-, and 5-year survival outcomes (overall survival [OS] and/or DFS) were comparable in both groups.
Compared with OMLR, LMLR has short-term clinical advantages, including reduced blood loss, lower postsurgical morbidity, and shorter hospital stay in HCC, despite its longer operative time. Long-term oncological outcomes were comparable in both groups.
腹腔镜肝切除术(LLR)在近几十年来迅速得到应用。尽管多位作者报道称,与开腹肝切除术(OLR)相比,LLR 在治疗肝细胞癌(HCC)方面具有更高的安全性和疗效,但腹腔镜(LMLR)和开腹(OMLR)肝切除术治疗 HCC 的效果仍未得到充分评估。本研究旨在验证 LMLR 治疗 HCC 比 OMLR 更安全、更有效的假设。
我们系统性地检索了 PubMed、科学引文索引、EMBASE 和 Cochrane 图书馆中截至 2018 年 3 月 31 日发表的关于 LMLR 和 OMLR 的比较队列和登记研究,并进行了荟萃分析。采用固定效应模型和随机效应模型生成汇总估计值。通过 Q 统计量评估异质性。
共纳入 9 项研究(1173 例患者)。尽管汇总数据显示,与 OMLR 相比,LMLR 的手术时间明显延长(加权均数差[WMD] 74.1,95%CI 35.1 至 113.1,P=0.0002),但术中出血量减少(WMD=-107.4,95%CI-179.0 至-35.7,P=0.003),术后并发症发生率较低(比值比[OR] 0.47,95%CI 0.35 至 0.63,P<0.0001),住院时间较短(WMD=-3.27,95%CI-4.72 至-1.81,P<0.0001)。尽管 LMLR 组患者 1 年无病生存率(DFS)增加(OR=1.55,95%CI 1.04 至 2.31,P=0.03),但两组患者的其他 1 年、3 年和 5 年生存结果(总生存[OS]和/或 DFS)无显著差异。
与 OMLR 相比,LMLR 治疗 HCC 具有短期临床优势,包括减少术中出血、降低术后并发症发生率和缩短住院时间,尽管手术时间较长。两组患者的长期肿瘤学结局无显著差异。