Medjeral-Thomas Nicholas R, Moffitt Hilary, Lomax-Browne Hannah J, Constantinou Nicholas, Cairns Tom, Cook H Terence, Pickering Matthew C
Centre for Inflammatory Disease, Division of Immunology and Inflammation, Department of Medicine, Imperial College London, UK.
Renal and Transplant Centre, Imperial College Healthcare NHS Trust, UK.
Kidney Int Rep. 2019 Jun 19;4(10):1387-1400. doi: 10.1016/j.ekir.2019.06.008. eCollection 2019 Oct.
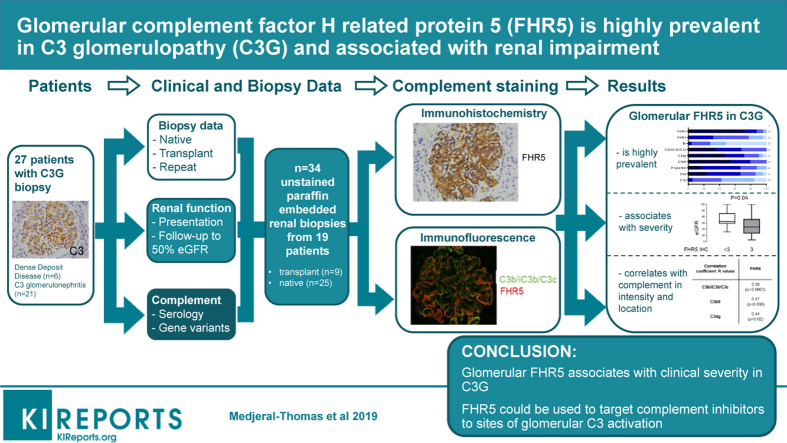
Therapeutic agents that target complement are increasingly available for glomerular diseases. However, the mechanisms linking glomerular complement deposition with inflammation and damage are incompletely understood. Complement factor H-related protein 5 (FHR5) interacts with complement C3 and is considered to promote activation. Circulating and glomerular FHR5 associates with IgA nephropathy and abnormal FHR5 associates with familial C3 glomerulopathy (C3G). We characterized glomerular FHR5 staining in C3G and assessed its relationships with histological features of glomerular injury and clinical outcome.
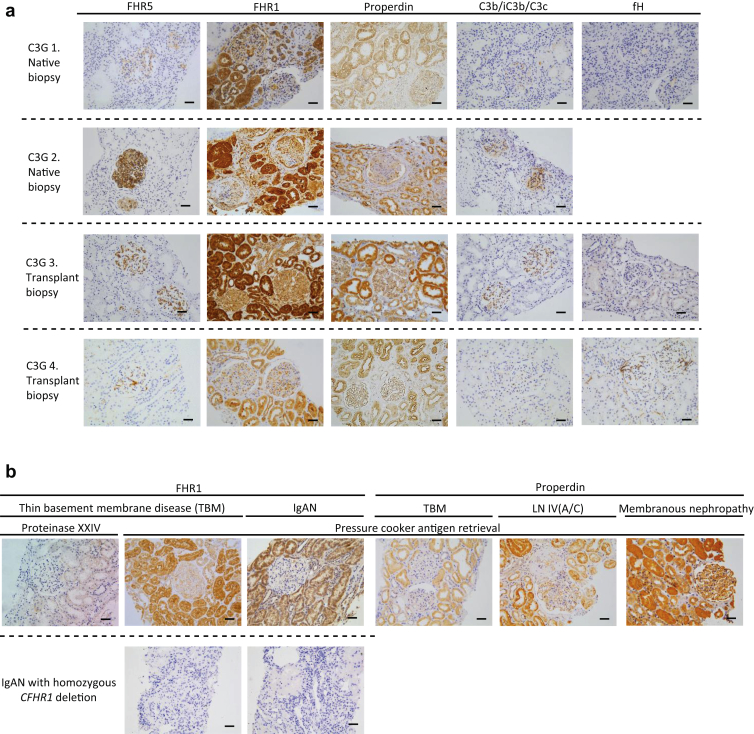
We developed FHR5 staining protocols for formalin-fixed paraffin-embedded (FFPE) renal tissue and applied them to surplus biopsy sections from a C3G cohort.
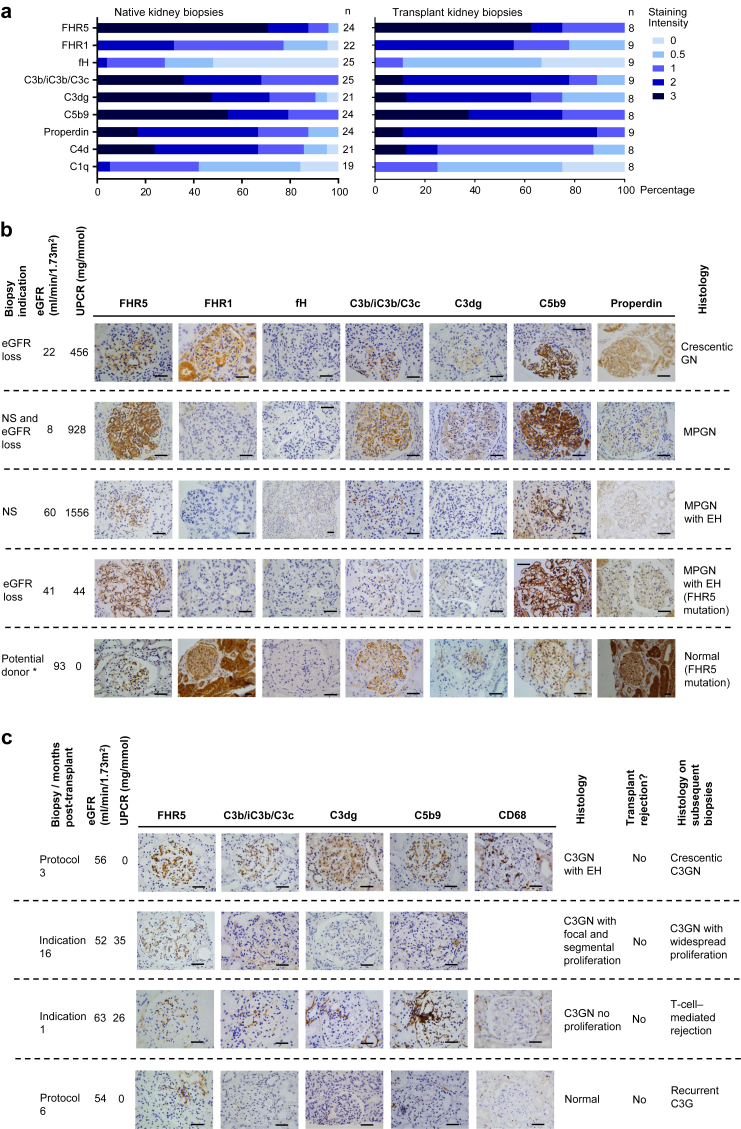
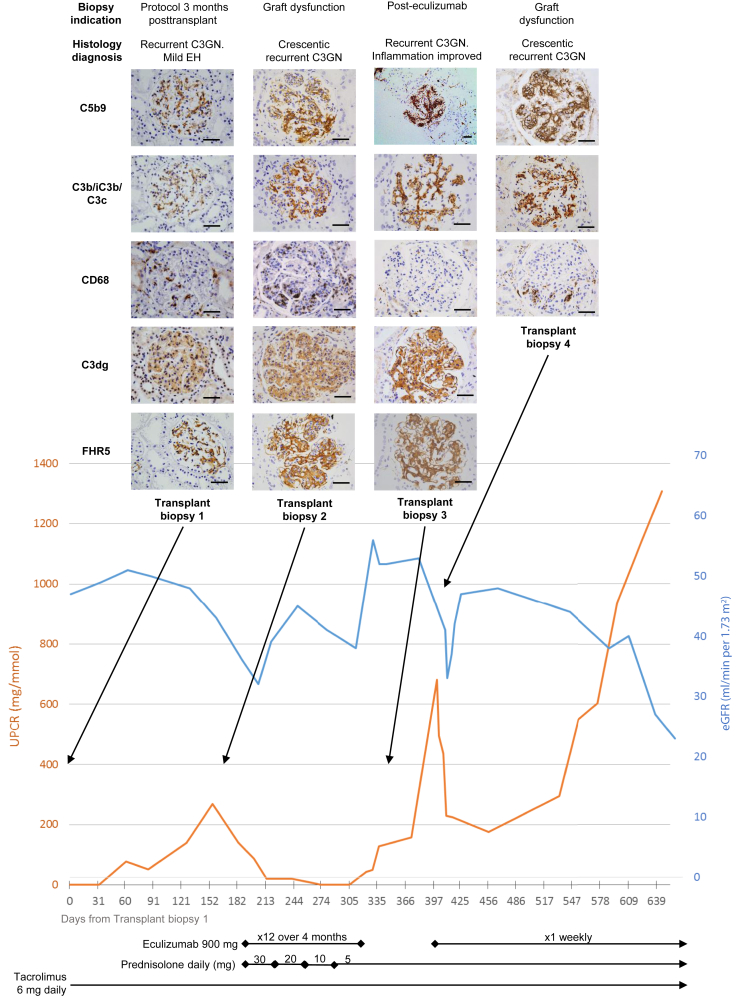
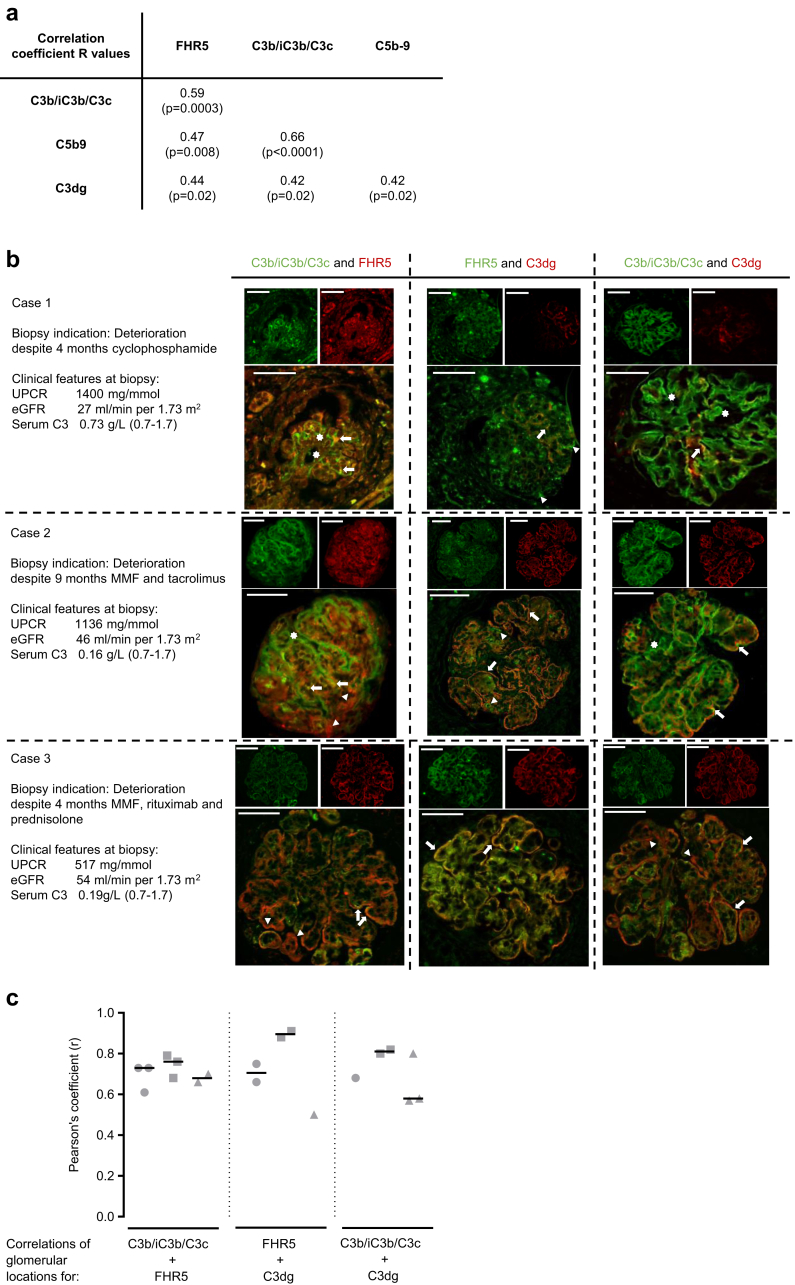
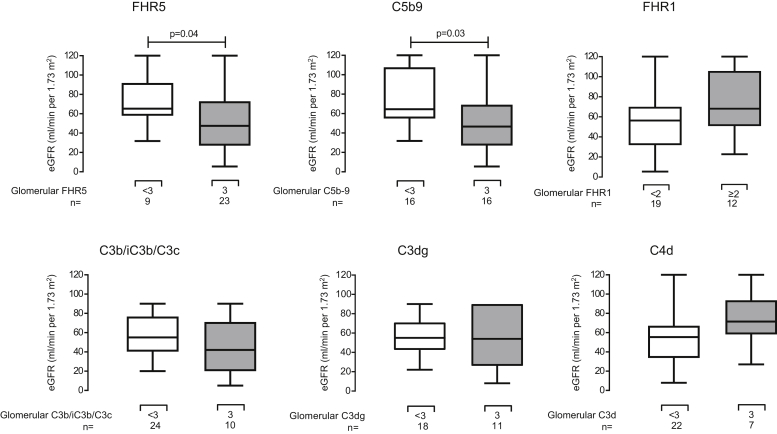
Glomerular FHR5 was highly prevalent in native and transplant C3G and correlated with glomerular C3 and C5b-9 staining. Glomerular FHR5 staining correlated negatively with estimated glomerular filtration rate (eGFR) ( = 0.04, difference of medians 19.7 ml/min per 1.73 m; 95% confidence interval [CI] 1.1-43.0) and positively with a membranoproliferative glomerulonephritis pattern at diagnostic biopsy (odds ratio 18; 95% CI 1.6-201; = 0.049). Glomerular FHR5 staining intensity positively correlated with glomerular complement C3b/iC3b/C3c (Pearson's correlation coefficient [] = 0.59; = 0.0008), C3dg ( = 0.47; = 0.02) and C5b9 ( = 0.44, = 0.02).
Glomerular FHR5 is highly prevalent in C3G, interacts with glomerular C3, and is associated with markers of disease severity. Glomerular FHR5 likely exacerbates complement-mediated glomerular damage in C3G and its interaction with glomerular complement might be exploited to target complement therapeutic agents.
针对补体的治疗药物越来越多地应用于肾小球疾病。然而,肾小球补体沉积与炎症和损伤之间的联系机制尚未完全明确。补体因子H相关蛋白5(FHR5)与补体C3相互作用,被认为可促进补体激活。循环和肾小球中的FHR5与IgA肾病相关,异常的FHR5与家族性C3肾小球病(C3G)相关。我们对C3G中肾小球FHR5染色进行了特征分析,并评估了其与肾小球损伤组织学特征及临床结局的关系。
我们开发了针对福尔马林固定石蜡包埋(FFPE)肾组织的FHR5染色方案,并将其应用于C3G队列的剩余活检切片。
肾小球FHR5在原发性和移植性C3G中高度普遍,且与肾小球C3和C5b-9染色相关。肾小球FHR5染色与估计肾小球滤过率(eGFR)呈负相关(r = 0.04,中位数差异为每1.73 m² 19.7 ml/min;95%置信区间[CI] 1.1 - 43.0),与诊断性活检时的膜增生性肾小球肾炎模式呈正相关(优势比18;95% CI 1.6 - 201;r = 0.049)。肾小球FHR5染色强度与肾小球补体C3b/iC3b/C3c(皮尔逊相关系数[r] = 0.59;P = 0.0008)、C3dg(r = 0.47;P = 0.02)和C5b9(r = 0.44,P = 0.02)呈正相关。
肾小球FHR5在C3G中高度普遍,与肾小球C3相互作用,并与疾病严重程度标志物相关。肾小球FHR5可能会加剧C3G中补体介导的肾小球损伤,其与肾小球补体的相互作用可能有助于靶向补体治疗药物。