Department of Neurology University of Alabama at Birmingham AL.
Department of Data Science and Medicine University of Mississippi Medical Center Jackson MS.
J Am Heart Assoc. 2019 Nov 19;8(22):e012874. doi: 10.1161/JAHA.119.012874. Epub 2019 Nov 8.
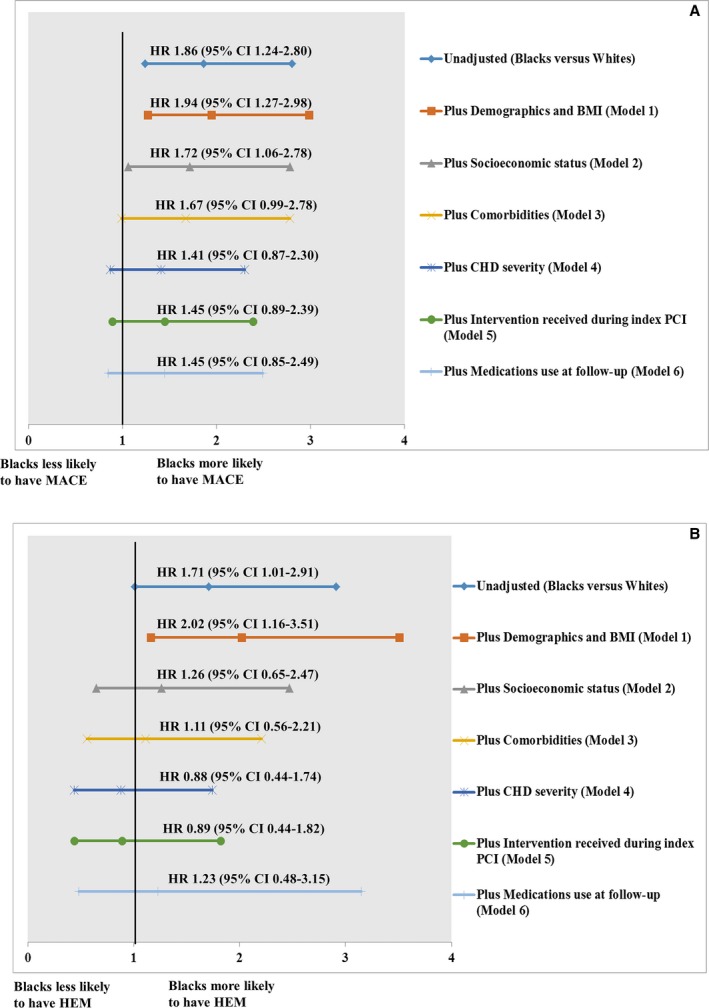
Background Data on racial disparities in major adverse cardiovascular events (MACE) and major hemorrhage (HEM) after percutaneous coronary intervention are limited. Factors contributing to these disparities are unknown. Methods and Results PRiME-GGAT (Pharmacogenomic Resource to Improve Medication Effectiveness-Genotype-Guided Antiplatelet Therapy) is a prospective cohort. Patients aged ≥18 years undergoing percutaneous coronary intervention were enrolled and followed for up to 1 year. Racial disparities in risk of MACE and HEM were assessed using an incident rate ratio. Sequential cumulative adjustment analyses were performed to identify factors contributing to these disparities. Data from 919 patients were included in the analysis. Compared with white patients, black patients (n=203; 22.1% of the cohort) were younger and were more likely to be female, to be a smoker, and to have higher body mass index, lower socioeconomic status, higher prevalence of diabetes mellitus and moderate to severe chronic kidney disease, and presentation with acute coronary syndrome and to undergo urgent percutaneous coronary intervention. The incident rates of MACE (34.1% versus 18.2% per 100 person-years, <0.001) and HEM (17.7% versus 10.3% per 100 person-years, =0.02) were higher in black patients. The incident rate ratio was 1.9 (95% CI, 1.3-2.6; <0.001) for MACE and 1.7 (95% CI, 1.1-2. 7; =0.02) for HEM. After adjustment for nonclinical and clinical factors, black race was not significantly associated with outcomes. Rather, differences in socioeconomic status, comorbidities, and coronary heart disease severity were attributed to racial disparities in outcomes. Conclusions Despite receiving similar treatment, racial disparities in MACE and HEM still exist. Opportunities exist to narrow these disparities by mitigating the identified contributors.
背景 关于经皮冠状动脉介入治疗后主要不良心血管事件(MACE)和大出血(HEM)的种族差异的数据有限。导致这些差异的因素尚不清楚。
方法和结果 PRiME-GGAT(改善药物疗效的药物基因组学资源-基于基因型的抗血小板治疗)是一项前瞻性队列研究。招募了年龄≥18 岁接受经皮冠状动脉介入治疗的患者,并随访了长达 1 年。使用发病率比评估 MACE 和 HEM 风险的种族差异。进行了连续累积调整分析,以确定导致这些差异的因素。对 919 例患者的数据进行了分析。与白人患者相比,黑人患者(n=203;队列的 22.1%)年龄更小,更可能是女性,是吸烟者,体重指数更高,社会经济地位较低,糖尿病和中重度慢性肾脏病的患病率更高,表现为急性冠状动脉综合征,并接受紧急经皮冠状动脉介入治疗。MACE(每 100 人年 34.1%与 18.2%,<0.001)和 HEM(每 100 人年 17.7%与 10.3%,=0.02)的发生率黑人患者更高。MACE 的发病率比为 1.9(95%CI,1.3-2.6;<0.001),HEM 的发病率比为 1.7(95%CI,1.1-2.7;=0.02)。在调整了非临床和临床因素后,黑人种族与结局之间没有显著关联。相反,社会经济地位、合并症和冠心病严重程度的差异归因于结局的种族差异。
结论 尽管接受了相似的治疗,但 MACE 和 HEM 仍存在种族差异。通过减轻已确定的促成因素,有机会缩小这些差异。