National Perinatal Epidemiology Unit, Nuffield Department of Population Health, University of Oxford, Oxford, United Kingdom.
Department of Obstetrics and Gynaecology, Leiden University Medical Centre, Leiden, the Netherlands.
PLoS Med. 2019 Nov 12;16(11):e1002962. doi: 10.1371/journal.pmed.1002962. eCollection 2019 Nov.
Amniotic fluid embolism (AFE) remains one of the principal reported causes of direct maternal mortality in high-income countries. However, obtaining robust information about the condition is challenging because of its rarity and its difficulty to diagnose. This study aimed to pool data from multiple countries in order to describe risk factors, management, and outcomes of AFE and to explore the impact on the findings of considering United Kingdom, international, and United States AFE case definitions.
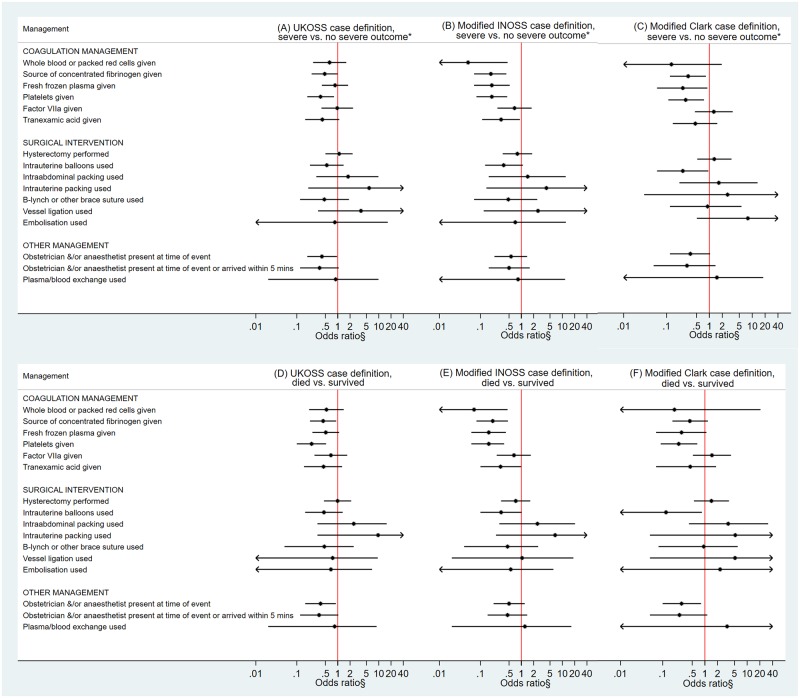
A population-based cohort and nested case-control study was conducted using the International Network of Obstetric Survey Systems (INOSS). Secondary data on women with AFE (n = 99-218, depending on case definition) collected prospectively in population-based studies conducted in Australia, France, the Netherlands, Slovakia, and the UK were pooled along with secondary data on a sample of control women (n = 4,938) collected in Australia and the UK. Risk factors for AFE were investigated by comparing the women with AFE in Australia and the UK with the control women identified in these countries using logistic regression. Factors associated with poor maternal outcomes (fatality and composite of fatality or permanent neurological injury) amongst women with AFE from each of the countries were investigated using logistic regression or Wilcoxon rank-sum test. The estimated incidence of AFE ranged from 0.8-1.8 per 100,000 maternities, and the proportion of women with AFE who died or had permanent neurological injury ranged from 30%-41%, depending on the case definition. However, applying different case definitions did not materially alter findings regarding risk factors for AFE and factors associated with poor maternal outcomes amongst women with AFE. Using the most liberal case definition (UK) and adjusting for the severity of presentation when appropriate, women who died were more likely than those who survived to present with cardiac arrest (89% versus 40%, adjusted odds ratio [aOR] 10.58, 95% confidence interval [CI] 3.93-28.48, p < 0.001) and less likely to have a source of concentrated fibrinogen (40% versus 56%, aOR 0.44, 95% CI 0.21-0.92, p = 0.029) or platelets given (24% versus 49%, aOR 0.23, 95% CI 0.10-0.52, p < 0.001). They also had a lower dose of tranexamic acid (median dose 0.7 g versus 2 g, p = 0.035) and were less likely to have had an obstetrician and/or anaesthetist present at the time of the AFE (61% versus 75%, aOR 0.38, 95% CI 0.16-0.90, p = 0.027). Limitations of the study include limited statistical power to examine factors associated with poor maternal outcome and the potential for residual confounding or confounding by indication.
The findings of our study suggest that when an AFE is suspected, initial supportive obstetric care is important, but having an obstetrician and/or anaesthetist present at the time of the AFE event and use of interventions to correct coagulopathy, including the administration of an adequate dose of tranexamic acid, may be important to improve maternal outcome. Future research should focus on early detection of the coagulation deficiencies seen in AFE alongside the role of tranexamic acid and other coagulopathy management strategies.
羊水栓塞(AFE)仍然是高收入国家产妇直接死亡的主要报告原因之一。然而,由于其罕见性和诊断困难,获得有关该病的可靠信息具有挑战性。本研究旨在汇集来自多个国家的数据,以描述 AFE 的危险因素、管理和结局,并探讨考虑英国、国际和美国 AFE 病例定义对研究结果的影响。
本研究采用国际产科调查系统网络(INOSS)进行了一项基于人群的队列和嵌套病例对照研究。在澳大利亚、法国、荷兰、斯洛伐克和英国进行的前瞻性人群研究中收集了 AFE 患者(取决于病例定义,n=99-218)的二级数据,并与澳大利亚和英国收集的对照组女性(n=4938)的二级数据进行了汇总。采用逻辑回归比较澳大利亚和英国的 AFE 患者与这些国家的对照组女性,以研究 AFE 的危险因素。采用逻辑回归或 Wilcoxon 秩和检验,研究了每个国家 AFE 患者中与不良母婴结局(死亡和死亡或永久性神经损伤的复合结局)相关的因素。根据病例定义的不同,AFE 的估计发病率为 0.8-1.8/100,000 例分娩,AFE 患者中死亡或发生永久性神经损伤的比例为 30%-41%。然而,应用不同的病例定义并不会改变关于 AFE 的危险因素和与 AFE 患者不良母婴结局相关的因素的研究结果。当适当时,使用最宽松的病例定义(英国)并调整表现的严重程度,与存活的患者相比,死亡的患者更有可能出现心脏骤停(89%对 40%,调整后的优势比[aOR]10.58,95%置信区间[CI]3.93-28.48,p<0.001),更不可能有浓缩纤维蛋白原的来源(40%对 56%,aOR 0.44,95%CI 0.21-0.92,p=0.029)或血小板输注(24%对 49%,aOR 0.23,95%CI 0.10-0.52,p<0.001)。他们还接受了较低剂量的氨甲环酸(中位数剂量 0.7 g 对 2 g,p=0.035),并且在 AFE 发生时产科医生和/或麻醉师在场的可能性较低(61%对 75%,aOR 0.38,95%CI 0.16-0.90,p=0.027)。研究的局限性包括检查不良母婴结局相关因素的统计能力有限,以及潜在的残余混杂或指示性混杂的可能性。
本研究结果表明,当怀疑发生 AFE 时,初始的支持性产科护理很重要,但在 AFE 发生时产科医生和/或麻醉师在场以及使用干预措施纠正凝血功能障碍,包括给予足够剂量的氨甲环酸,可能对改善母婴结局很重要。未来的研究应重点关注 AFE 中所见凝血缺陷的早期检测,以及氨甲环酸和其他凝血功能障碍管理策略的作用。