Department of Pediatrics, Shandong Provincial Hospital Affiliated to Shandong University, 9677 Jingshi Road, Jinan, 250014, Shandong, China.
BMC Pediatr. 2019 Nov 14;19(1):441. doi: 10.1186/s12887-019-1819-6.
Pituitary tumors and/or their treatment are associated with multiple pituitary hormone deficiency (MPHD) in adults, but the distinct pituitary hormone profile of MPHD in Chinese children and adolescents remains unclear.
Patients with MPHD were divided into four groups according to their MRI results: 1) pituitary stalk interruption syndrome (PSIS); 2) hypoplasia; 3) normal; and 4) tumor survivor.
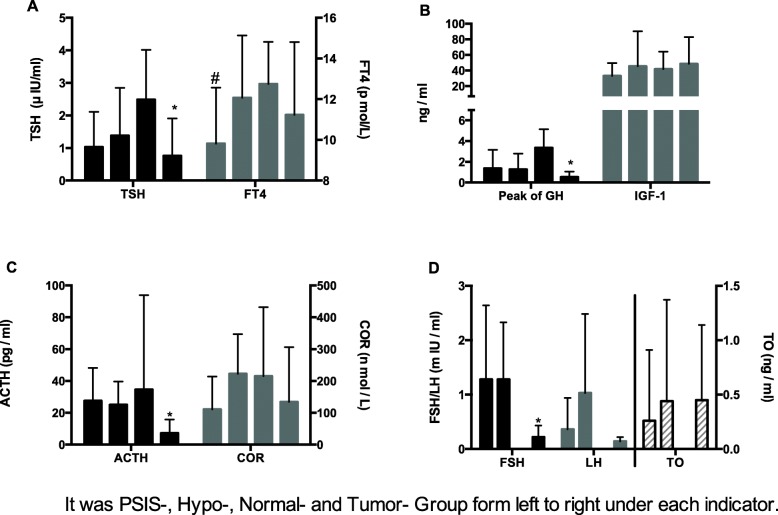
Among the 184 patients, 93 patients (50.5%) were with PSIS, 24 (13.0%) had hypoplastic pituitary gland, 10 (5.4%) patients were normal, and 57 (31.0%) were tumor survivors. There was an association between abnormal fetal position and PSIS (P ≤ 0.001). The CA/BA in PSIS, hypoplasia, normal, tumor survivor groups were 2.27 ± 1.05, 1.48 ± 0.39, 1.38 ± 0.57, 1.49 ± 0.33, and HtSDS were - 3.94 ± 1.39, - 2.89 ± 1.09, - 2.50 ± 1.05, - 1.38 ± 1.63. Patients in PSIS group had the largest CA/BA (P ≤ 0.001 vs. hypoplasia group, P = 0.009 vs. normal group, P ≤ 0.001 vs. tumor survivors) and lowest HtSDS (P ≤ 0.001 vs. hypoplasia group, P = 0.003 vs. normal group, P ≤ 0.001 vs. tumor survivors). The levels of TSH in the PSIS, hypoplasia, normal, and tumor survivor groups were 1.03 ± 1.08 (P = 0.149 vs. tumor survivors), 1.38 ± 1.47 (P = 0.045 vs. tumor survivors), 2.49 ± 1.53 (P < 0.001 vs. tumor survivors), and 0.76 ± 1.15 μIU/ml. The levels of GH peak in PSIS, hypoplasia, normal, tumor survivor groups were 1.37 ± 1.78, 1.27 ± 1.52, 3.36 ± 1.79, 0.53 ± 0.52 ng/ml and ACTH were 27.50 ± 20.72, 25.05 ± 14.64, 34.61 ± 59.35, 7.19 ± 8.63 ng/ml. Tumor survivors had the lowest levels of GH peak (P ≤ 0.001 vs. PSIS group, P = 0.002 vs. hypoplasia group, P ≤ 0.001 vs. normal group) and ACTH (all the P ≤ 0.001 vs. the other three groups).
The frequency of PSIS is high among children and adolescents with MPHD. The severity of hormone deficiencies in patients with MPHD was more important in the tumor survivor group compared with the other groups.
垂体肿瘤及其治疗与成年人的多种垂体激素缺乏症(MPHD)有关,但中国儿童和青少年 MPHD 的独特垂体激素特征仍不清楚。
根据 MRI 结果,将 MPHD 患者分为四组:1)垂体柄中断综合征(PSIS);2)发育不良;3)正常;和 4)肿瘤幸存者。
在 184 例患者中,93 例(50.5%)存在 PSIS,24 例(13.0%)存在垂体发育不良,10 例(5.4%)患者正常,57 例(31.0%)为肿瘤幸存者。异常胎儿位置与 PSIS 有关(P≤0.001)。PSIS、发育不良、正常、肿瘤幸存者组的 CA/BA 分别为 2.27±1.05、1.48±0.39、1.38±0.57、1.49±0.33,HtSDS 分别为-3.94±1.39、-2.89±1.09、-2.50±1.05、-1.38±1.63。PSIS 组患者的 CA/BA 最大(P≤0.001 与发育不良组,P=0.009 与正常组,P≤0.001 与肿瘤幸存者),HtSDS 最低(P≤0.001 与发育不良组,P=0.003 与正常组,P≤0.001 与肿瘤幸存者)。PSIS、发育不良、正常、肿瘤幸存者组 TSH 水平分别为 1.03±1.08(P=0.149 与肿瘤幸存者)、1.38±1.47(P=0.045 与肿瘤幸存者)、2.49±1.53(P<0.001 与肿瘤幸存者)和 0.76±1.15 μIU/ml。PSIS、发育不良、正常、肿瘤幸存者组 GH 峰值水平分别为 1.37±1.78、1.27±1.52、3.36±1.79、0.53±0.52ng/ml,ACTH 分别为 27.50±20.72、25.05±14.64、34.61±59.35、7.19±8.63ng/ml。肿瘤幸存者的 GH 峰值(P≤0.001 与 PSIS 组,P=0.002 与发育不良组,P≤0.001 与正常组)和 ACTH(所有 P≤0.001 与其他三组)水平最低。
儿童和青少年 MPHD 中 PSIS 的发生率较高。与其他三组相比,MPHD 患者的激素缺乏严重程度在肿瘤幸存者组更为重要。