Vidal Liat, Gafter-Gvili Anat, Dreyling Martin, Ghielmini Michele, Witzens-Harig Mathias, Shpilberg Ofer, Unterhalt Michael, Rummel Mathias, Gurion Ronit
Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv.
Institute of Hematology, Davidoff Center, Beilinson Hospital, Rabin Medical Center.
Hemasphere. 2018 Jul 27;2(4):e136. doi: 10.1097/HS9.0000000000000136. eCollection 2018 Aug.
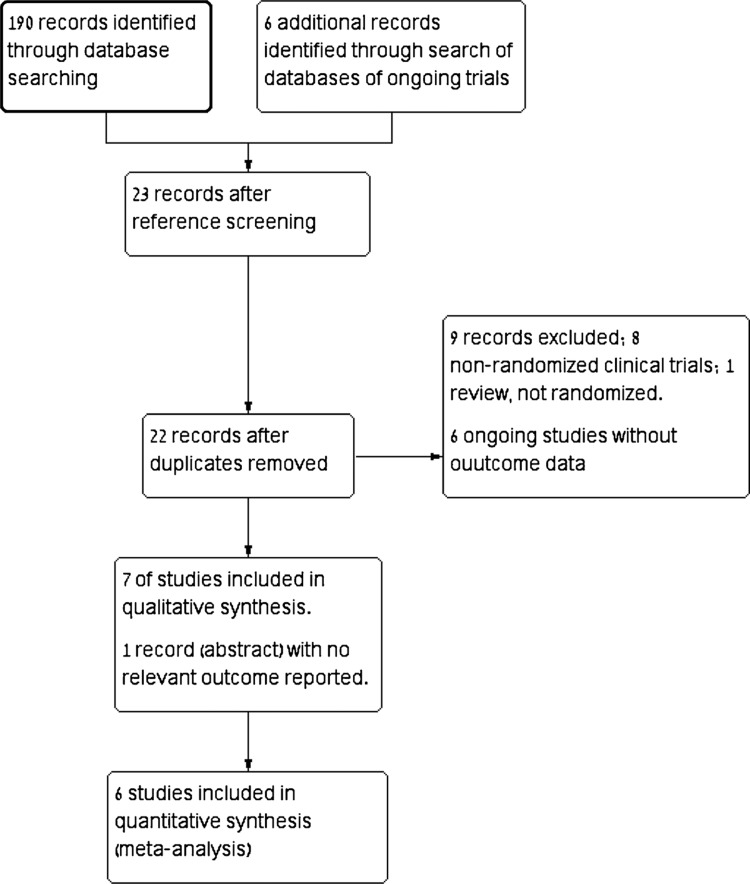
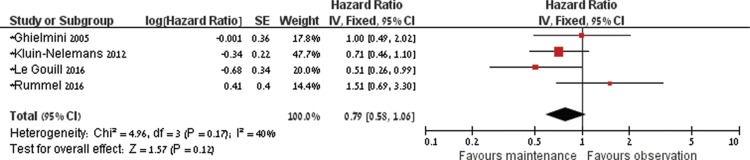
Current treatment of patient with mantle cell lymphoma (MCL) is insufficient and does not result in cure. To assess the efficacy and safety of maintenance therapy for patients with MCL, we performed a systematic review and meta-analysis of randomized controlled trials. Six trials randomizing 858 patients were included in the meta-analysis. In 5 trials, maintenance therapy consisted of rituximab. The pooled hazard ratio (HR) of death with rituximab maintenance compared to observation was 0.79, 95% CI 0.58 to 1.06 (4 trials, 737 patients). Progression free survival was longer with rituximab maintenance in each of the trials and in the pooled analysis (HR 0.58, 95% CI 0.45-0.73). The risk of neutropenia was higher with maintenance compared to observation risk ratio (RR) 1.31, 95% CI 1.03 to 1.66. None of the trials reported on quality of life outcomes. The grade 3 to 4 infection rate was 7% in each of the treatment groups. The risk of grade 3 to 4 infection was not affected by allocation to maintenance. Rituximab maintenance is recommended after R-CHOP or R-cytarabine-containing induction in the frontline setting for transplant eligible and ineligible patients, and after R-CHOP in the relapse setting. It is unclear if maintenance is of benefit after different induction chemotherapy such as bendamustine or fludarabine. It is too early to conclude on other type of maintenance for MCL patients.
目前套细胞淋巴瘤(MCL)患者的治疗并不充分,无法实现治愈。为评估MCL患者维持治疗的疗效和安全性,我们对随机对照试验进行了系统评价和荟萃分析。荟萃分析纳入了6项随机分配858例患者的试验。在5项试验中,维持治疗方案为利妥昔单抗。与观察相比,利妥昔单抗维持治疗的汇总死亡风险比(HR)为0.79,95%置信区间为0.58至1.06(4项试验,737例患者)。在每项试验及汇总分析中,利妥昔单抗维持治疗的无进展生存期均更长(HR 0.58,95%置信区间0.45 - 0.73)。与观察相比,维持治疗的中性粒细胞减少风险更高,风险比(RR)为1.31,95%置信区间为1.03至1.66。没有试验报告生活质量结果。各治疗组3至4级感染率均为7%。分配至维持治疗组对3至4级感染风险无影响。对于适合和不适合移植的一线患者,在含R-CHOP或含阿糖胞苷的诱导治疗后,以及复发患者在R-CHOP治疗后,推荐使用利妥昔单抗维持治疗。目前尚不清楚在使用苯达莫司汀或氟达拉滨等不同诱导化疗后维持治疗是否有益。对于MCL患者的其他类型维持治疗,现在下结论还为时过早。