Asan Medical Center, University of Ulsan College of Medicine, Seoul, South Korea.
Fudan University Shanghai Cancer Center, Shanghai, China.
J Hematol Oncol. 2020 Mar 17;13(1):21. doi: 10.1186/s13045-020-00855-9.
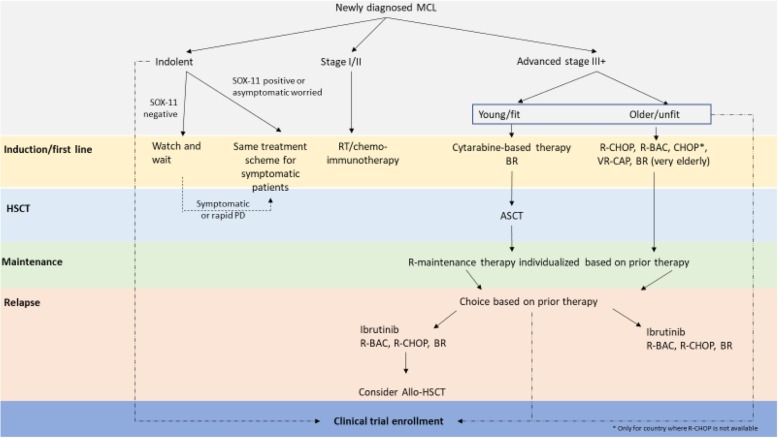
Mantle cell lymphoma (MCL) is a B cell malignancy that can be aggressive and with a poor prognosis; the clinical course is heterogeneous. The epidemiology of MCL in Asia is not well documented but appears to comprise 2-6% of all lymphoma cases based on available data, with variation observed between countries. Although international guidelines are available for the treatment of MCL, there is a lack of published data or guidance on the clinical characteristics and management of MCL in patient populations from Asia. This paper aims to review the available treatment and, where clinical gaps exist, provide expert consensus from the Asian Lymphoma Study Group (ALSG) on appropriate MCL management in Asia. BODY: Management strategies for MCL are patient- and disease stage-specific and aim to achieve balance between efficacy outcomes and toxicity. For asymptomatic patients with clearly indolent disease, observation may be an appropriate strategy. For stage I/II disease, following international guidelines is appropriate, which include either a short course of conventional chemotherapy followed by consolidated radiotherapy, less aggressive chemotherapy regimens, or a combination of these approaches. For advanced disease, the approach is based on the age and fitness of the patient. For young, fit patients, the current practice for induction therapy differs across Asia, with cytarabine having an important role in this setting. Hematopoietic stem cell transplantation (HSCT) may be justified in selected patients because of the high relapse risk. In elderly patients, specific chemoimmunotherapy regimens available in each country/region are a treatment option. For maintenance therapy after first-line treatment, the choice of approach should be individualized, with cost being an important consideration within Asia. For relapsed/refractory disease, ibrutinib should be considered as well as other follow-on compounds, if available.
Asian patient-specific data for the treatment of MCL are lacking, and the availability of treatment options differs between country/region within Asia. Therefore, there is no clear one-size-fits-all approach and further investigation on the most appropriate sequence of treatment that should be considered for this heterogeneous disease.
套细胞淋巴瘤(MCL)是一种侵袭性和预后不良的 B 细胞恶性肿瘤;其临床过程具有异质性。亚洲的 MCL 流行病学尚未得到很好的记录,但根据现有数据,该病占所有淋巴瘤病例的 2-6%,不同国家之间存在差异。尽管有治疗 MCL 的国际指南,但亚洲患者人群的 MCL 临床特征和管理方面缺乏已发表的数据或指导。本文旨在回顾现有治疗方法,并在存在临床空白的情况下,由亚洲淋巴瘤研究组(ALSG)就亚洲 MCL 的适当管理提供专家共识。
MCL 的管理策略是基于患者和疾病分期的,旨在在疗效结果和毒性之间取得平衡。对于无症状且疾病明显惰性的患者,观察可能是一种合适的策略。对于 I/II 期疾病,遵循国际指南是合适的,包括短期常规化疗后联合巩固放疗、较不激进的化疗方案或这些方法的组合。对于晚期疾病,方法取决于患者的年龄和健康状况。对于年轻、健康的患者,亚洲各地的诱导治疗方法不同,阿糖胞苷在这种情况下具有重要作用。由于复发风险高,造血干细胞移植(HSCT)可能在某些患者中合理。在老年患者中,每个国家/地区都有特定的化疗免疫治疗方案可供选择。对于一线治疗后的维持治疗,选择哪种方法应个体化,成本是亚洲需要考虑的重要因素。对于复发/难治性疾病,应考虑使用伊布替尼以及其他后续化合物(如果有)。
亚洲缺乏治疗 MCL 的患者特异性数据,亚洲各国/地区的治疗方案可用性存在差异。因此,对于这种异质性疾病,没有明确的一刀切的方法,需要进一步研究应考虑的最合适的治疗顺序。