Zabeirou Abdoul Aliou, Belghali Houssam, Souiki Tarek, Ibn Majdoub Karim, Toughrai Imane, Mazaz Khalid
Department of General and Visceral Surgery, Hassan II University Hospital of Fez, 30050, Fez, Morocco.
Faculty of Medicine and Pharmacy, Sidi Mohamed Ben Abdellah University of Fez, 30050, Fez, Morocco.
Ann Med Surg (Lond). 2019 Oct 31;48:69-72. doi: 10.1016/j.amsu.2019.10.021. eCollection 2019 Dec.
Cecal volvulus is an uncommon cause of intestinal obstruction due to an axial twist of the caecum, ascending colon and terminal ileum around the mesenteric pedicle. It is responsible for 1%-1.5 of all intestinal obstructions in adult. The clinical signs may be highly variables and can be responsible of delays in diagnostic and treatment. The delay in diagnosis leads to intestinal necrosis or perforation. The mortality ranges from 10 to 40% depending on the presence of a viable or gangrenous intestine.
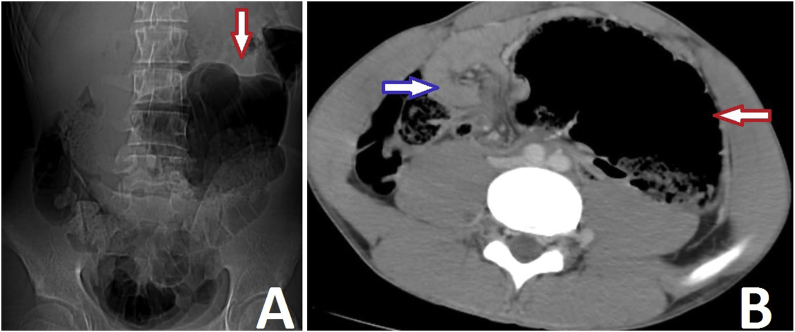
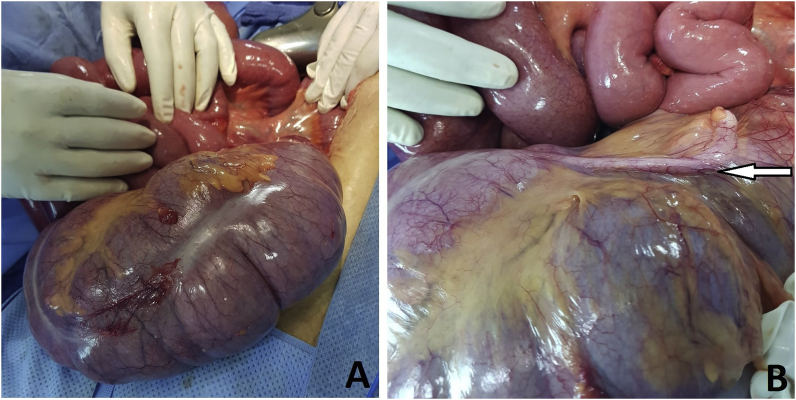
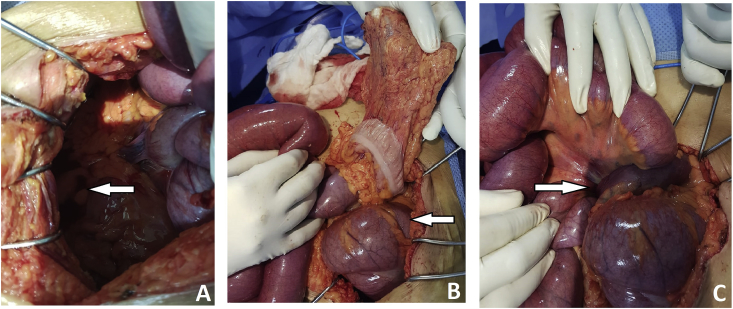
A 64 year old woman admitted the emergency department for acute bowel obstruction. Clinical examination found typically acute bowel obstruction signs. Plain radiography showed dilated gas-filled segment of the colon in the left side of abdomen and volvulus of cecum was suspected. Enhanced abdominal CT scan confirmed the diagnosis. Emergency exploratory laparotomy was performed and confirmed the cecal volvulus. A manual untwisting of volvulus and a Caecopexy were performed. The patient subsequently recovered uneventfully and was discharged on postoperative day 3.
The management of cecal volvulus requires prompt (emergency) diagnosis and prompt surgical intervention. Any delay in diagnosis may lead to intestinal necrosis or perforation and worsening the prognosis in patients who are generally elderly. Several authors reported a high mortality rate of cecal volvulus due to delay to diagnosis and surgical intervention.
The low incidence of this condition needs a high index of suspicion and emergency surgical management. Despite significant progress in medical imaging, the preoperative diagnosis of cecal volvulus is very difficult. As a result, the treatment is often delayed.
盲肠扭转是由于盲肠、升结肠和回肠末端围绕肠系膜蒂发生轴向扭转而导致肠梗阻的罕见原因。它占成人所有肠梗阻病例的1%-1.5%。临床症状可能差异很大,可能导致诊断和治疗延误。诊断延误可导致肠坏死或穿孔。根据肠管是否存活或已坏疽,死亡率在10%至40%之间。
一名64岁女性因急性肠梗阻入住急诊科。临床检查发现典型的急性肠梗阻体征。腹部平片显示左腹部结肠充气扩张段,怀疑有盲肠扭转。增强腹部CT扫描确诊。进行了急诊剖腹探查术,证实为盲肠扭转。进行了手动扭转复位和盲肠固定术。患者随后顺利康复,术后第3天出院。
盲肠扭转的治疗需要迅速(急诊)诊断和及时的手术干预。任何诊断延误都可能导致肠坏死或穿孔,并使通常为老年人的患者预后恶化。几位作者报告称,由于诊断和手术干预延误,盲肠扭转的死亡率很高。
这种疾病的低发病率需要高度的怀疑指数和急诊手术治疗。尽管医学影像学取得了重大进展,但盲肠扭转的术前诊断仍然非常困难。因此,治疗往往会延迟。