Toth Peter P, Fazio Sergio, Wong Nathan D, Hull Michael, Nichols Gregory A
Ciccarone Centre for the Prevention of Cardiovascular Disease, Johns Hopkins University School of Medicine, Baltimore, Maryland, United States.
CGH Medical Center, Sterling, Illinois, United States.
Diabetes Obes Metab. 2020 Mar;22(3):279-289. doi: 10.1111/dom.13921. Epub 2019 Dec 26.
To describe the real-world prevalence and consequences of hypertriglyceridaemia.
We searched two large patient databases, the National Health and Nutrition Examination Survey (NHANES) database (2007-2014) and the Optum Research Database, as well as electronic medical records from two Kaiser Permanente regions.
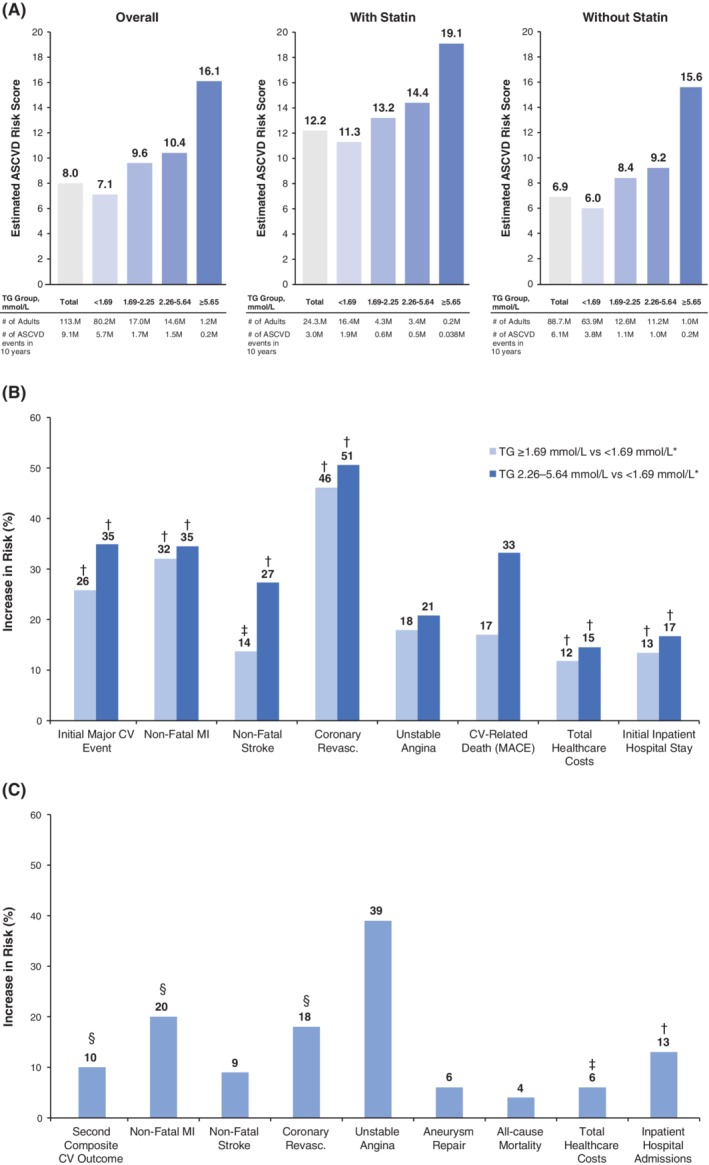
The NHANES data showed that ~26% of US adults, including nearly one-third of statin users, had at least borderline hypertriglyceridaemia (triglycerides [TGs] ≥1.69 mmol/L), and ~40% of adults with diabetes had levels of ≥150 mg/dL despite statin use. The Optum analyses demonstrated that those with TG levels ≥1.69 mmol/L who were on statins had a significantly increased risk of composite initial major cardiovascular (CV) events (hazard ratio [HR] 1.26, 95% confidence interval [CI] 1.19-1.34; P < 0.001 vs. patients with TGs <150 mg/dL). This was accompanied by increased healthcare utilization and direct healthcare costs (HR 1.12, 95% CI 1.08-1.16; P < 0.001). In the analyses of the Kaiser Permanente records, patients with diabetes and TG levels 2.26-5.64 mmol/L had significantly higher adjusted incidence rates of non-fatal myocardial infarction (rate ratio 1.30, 95% CI 1.08-1.58; P = 0.006), non-fatal stroke (rate ratio 1.23; 95% CI 1.01-1.49; P = 0.037) and coronary revascularization (rate ratio 1.21; 95% CI 1.02-1.43; P = 0.027), but not unstable angina (rate ratio 1.33; 95% CI 0.87-2.03; P = 0.185) compared with patients with TG levels <1.69 mmol/L.
Real-world analyses suggest that elevated TGs are prevalent and commonly associated with increased CV risk. CV outcomes trials in patients with established hypertriglyceridaemia will clarify whether strategies to reduce TG levels can ameliorate residual CV risk in patients taking statins.
描述高甘油三酯血症在现实世界中的患病率及其后果。
我们检索了两个大型患者数据库,即美国国家健康与营养检查调查(NHANES)数据库(2007 - 2014年)和Optum研究数据库,以及来自凯撒医疗机构两个地区的电子病历。
NHANES数据显示,约26%的美国成年人,包括近三分之一的他汀类药物使用者,至少有边缘性高甘油三酯血症(甘油三酯[TGs]≥1.69 mmol/L),并且约40%的糖尿病成年人尽管使用了他汀类药物,甘油三酯水平仍≥150 mg/dL。Optum分析表明,他汀类药物治疗的TG水平≥1.69 mmol/L的患者发生复合初始主要心血管(CV)事件的风险显著增加(风险比[HR] 1.26,95%置信区间[CI] 1.19 - 1.34;与TGs <150 mg/dL的患者相比,P < 0.001)。这伴随着医疗保健利用率和直接医疗成本的增加(HR 1.12,95% CI 1.08 - 1.16;P < 0.001)。在凯撒医疗机构记录的分析中,糖尿病且TG水平为2.26 - 5.64 mmol/L的患者,与TG水平<1.69 mmol/L的患者相比,非致命性心肌梗死的校正发病率显著更高(率比1.30,95% CI 1.08 - 1.58;P = 0.006),非致命性中风(率比1.23;95% CI 1.01 - 1.49;P =
0.037)和冠状动脉血运重建(率比1.21;95% CI 1.02 - 1.43;P = 0.027),但不稳定型心绞痛并非如此(率比1.33;95% CI 0.87 - 2.03;P = 0.185)。
现实世界分析表明,TG水平升高很普遍,且通常与心血管风险增加相关。针对已确诊高甘油三酯血症患者的心血管结局试验将阐明降低TG水平的策略是否能改善服用他汀类药物患者的残余心血管风险。