The Jockey Club School of Public Health and Primary Care, The Chinese University of Hong Kong, Hong Kong, SAR, People's Republic of China.
BMC Health Serv Res. 2019 Nov 21;19(1):875. doi: 10.1186/s12913-019-4707-8.
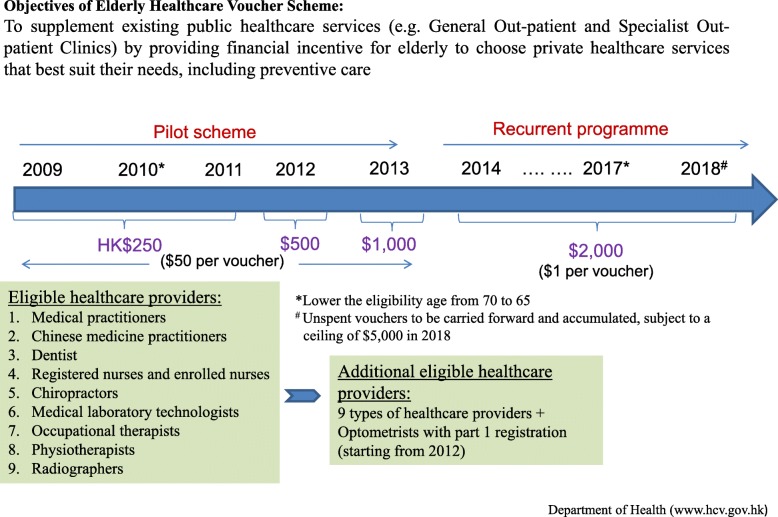
Vouchers are increasingly used as a demand-side subsidy to reduce financial hardship and improve quality of services. Elderly Healthcare Voucher Scheme has been introduced by the Hong Kong Government since 2009 to provide subsidy to elderly aged 65 and above to visit ten different types of private primary care providers for curative, preventive and chronic disease management. Several enhancements have been made over the past few years. This paper (as part of an evaluation study of this unique healthcare voucher scheme) aims to assess the long term impact of the voucher scheme in encouraging the use of primary care services.
Two rounds of cross-sectional survey among elderly in Hong Kong were conducted in 2010 and 2016. Propensity score matching and analysis were used to compare changes in perception and usage of vouchers over time.
61.5% of respondents in 2016 agreed "the scheme encourages me to use more private primary care services", a significant increase from 36.2% in 2010. Among those who agreed in 2016, the majority thought the voucher scheme would encourage them to use acute services (90.3%) in the private sector, rather than preventive care (40.3%) and chronic disease management (12.2%). Respondents also reported that their current usual choice of care was visiting "both public and private doctors" (61.9%), representing a significant increase (up from 48.4%) prior to their use of voucher.
The voucher scheme has encouraged the use of more private care services, particularly acute services rather than disease prevention or management of chronic disease. However, there needs to be caution that the untargeted and open-ended nature of voucher scheme could result in supply-induced demand which would affect long term financial sustainability. The dual utilization of health services in both the public and private sector may also compromise continuity and quality of care. The design of the voucher needs to be more specific, targeting prevention and chronic disease management rather than unspecified care which is mainly acute and episodic in order to maximize service delivery capacity as a whole for equitable access in universal health coverage and to contribute to a sustainable financing system.
凭证正被越来越多地用作需求方补贴,以减轻经济困难并提高服务质量。自 2009 年以来,香港政府推出了“长者医疗券计划”,为 65 岁及以上的老年人提供补贴,以让他们在十家不同类型的私人基层医疗提供者处接受治疗、预防和慢性病管理服务。近年来,该计划进行了多次改进。本文(作为对这项独特的医疗券计划进行评估研究的一部分)旨在评估该券计划在鼓励使用基层医疗服务方面的长期影响。
在 2010 年和 2016 年,对香港的老年人进行了两轮横断面调查。使用倾向评分匹配和分析来比较随时间推移对凭证的认知和使用的变化。
2016 年,61.5%的受访者同意“该计划鼓励我更多地使用私人基层医疗服务”,这一比例较 2010 年的 36.2%显著增加。在 2016 年同意的受访者中,大多数人认为券计划将鼓励他们在私营部门使用急性服务(90.3%),而不是预防保健(40.3%)和慢性病管理(12.2%)。受访者还报告称,他们目前通常的就诊选择是“同时看公营和私营医生”(61.9%),这一比例较使用券前的 48.4%显著增加。
券计划鼓励了更多私人护理服务的使用,特别是急性服务,而不是疾病预防或慢性病管理。然而,需要谨慎的是,券计划的无针对性和开放式性质可能导致供应诱导需求,从而影响长期财务可持续性。公私部门双重利用卫生服务也可能影响医疗服务的连续性和质量。券的设计需要更加具体,针对预防和慢性病管理,而不是非特定的护理,主要是急性和偶发性的,以便最大限度地提高整体服务交付能力,实现全民健康覆盖的公平获取,并为可持续的融资系统做出贡献。