Stirrup Oliver T, Sabin Caroline A, Phillips Andrew N, Williams Ian, Churchill Duncan, Tostevin Anna, Hill Teresa, Dunn David T
Institute for Global Health, University College London, London, UK.
Mortimer Market Centre, Central and North West London NHS Foundation Trust, London, UK.
J Virus Erad. 2019 Nov 4;5(4):204-211. doi: 10.1016/S2055-6640(20)30037-6.
The aim of this study was to investigate associations between baseline characteristics and CD4 cell count response on first-line antiretroviral therapy and risk of virological failure (VF) with or without drug resistance.
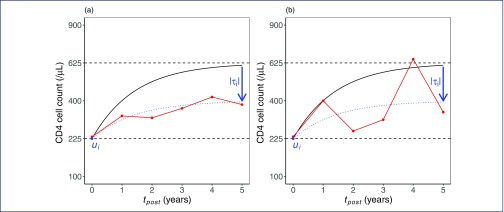
We conducted an analysis of UK Collaborative HIV Cohort data linked to the UK HIV Drug Resistance Database. Inclusion criteria were viral sequence showing no resistance prior to initiation of first-line efavirenz + tenofovir disoproxil fumarate + emtricitabine and virological suppression within 6 months. Outcomes of VF (≥200 copies/mL) with or without drug resistance were assessed using a competing risks approach fitted jointly with a model for CD4 cell count recovery. Hazard ratios for each VF outcome were estimated for baseline CD4 cell count and viral load and characteristics of CD4 cell count response using latent variables on a standard normal scale.
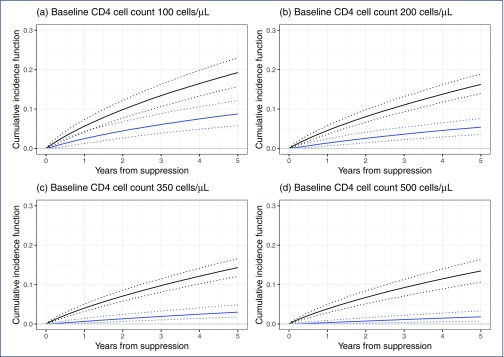
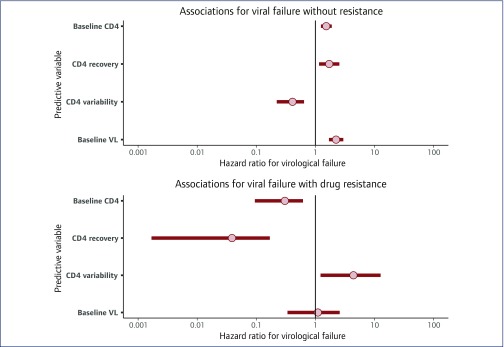
A total of 3640 people were included with 338 VF events; corresponding viral sequences were available in 134 with ≥1 resistance mutation in 36. VF with resistance was associated with lower baseline CD4 (0.30, 0.09-0.62), lower CD4 recovery (0.04, 0.00-0.17) and higher CD4 variability (4.40, 1.22-12.68). A different pattern of associations was observed for VF without resistance, but the strength of these results was less consistent across sensitivity analyses. Cumulative incidence of VF with resistance was estimated to be <2% at 3 years for baseline CD4 ≥350 cells/μL.
Lower baseline CD4 cell count and suboptimal CD4 recovery are associated with VF with drug resistance. People with low CD4 cell count before ART or with suboptimal CD4 recovery on treatment should be a priority for regimens with high genetic barrier to resistance.
本研究旨在调查一线抗逆转录病毒治疗时基线特征与CD4细胞计数反应之间的关联,以及有无耐药情况下病毒学失败(VF)的风险。
我们对与英国HIV耐药数据库相关联的英国协作HIV队列数据进行了分析。纳入标准为在开始一线依非韦伦+替诺福韦酯富马酸盐+恩曲他滨之前病毒序列无耐药性,且在6个月内实现病毒学抑制。使用竞争风险方法联合CD4细胞计数恢复模型评估有无耐药情况下的VF结局(≥200拷贝/mL)。使用标准正态尺度上的潜在变量估计每个VF结局的风险比,以分析基线CD4细胞计数、病毒载量以及CD4细胞计数反应特征。
共纳入3640人,发生338次VF事件;其中134人有相应病毒序列,36人有≥1个耐药突变。有耐药的VF与较低的基线CD4(0.30,0.09 - 0.62)、较低的CD4恢复(0.04,0.00 - 0.17)和较高的CD4变异性(4.40,1.22 - 12.68)相关。对于无耐药的VF观察到不同的关联模式,但这些结果在敏感性分析中的强度不太一致。对于基线CD4≥350细胞/μL的患者,3年时有耐药的VF累积发生率估计<2%。
较低的基线CD4细胞计数和次优的CD4恢复与有耐药的VF相关。在抗逆转录病毒治疗前CD4细胞计数低或治疗期间CD4恢复次优的患者,应优先使用对耐药具有高遗传屏障的治疗方案。