Lee Dohyeong, Yun Byung Cheol, Seo Kwang Il, Han Byung Hoon, Lee Sang Uk, Park Eun Taek, Lee Jin Wook, Jeong Joonho
Department of Internal Medicine, Kosin University College of Medicine, Busan, Korea.
Medicine (Baltimore). 2019 Dec;98(50):e18351. doi: 10.1097/MD.0000000000018351.
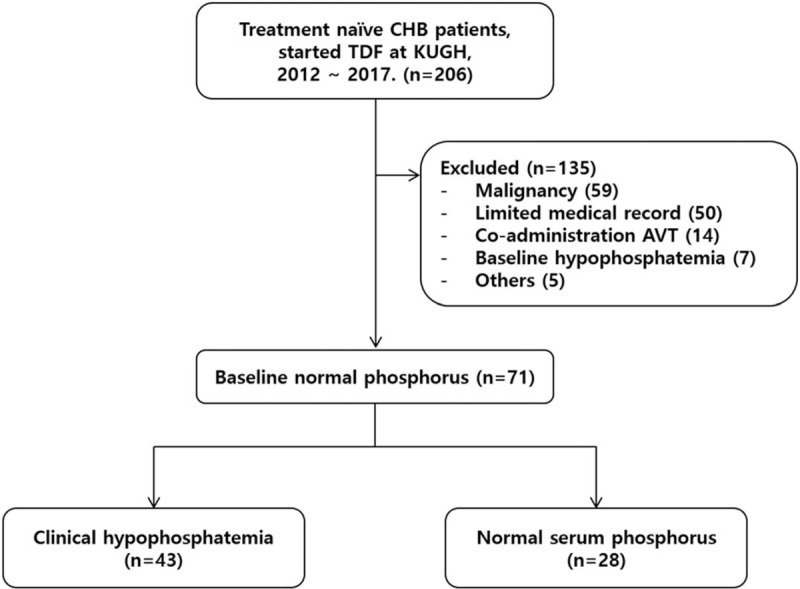
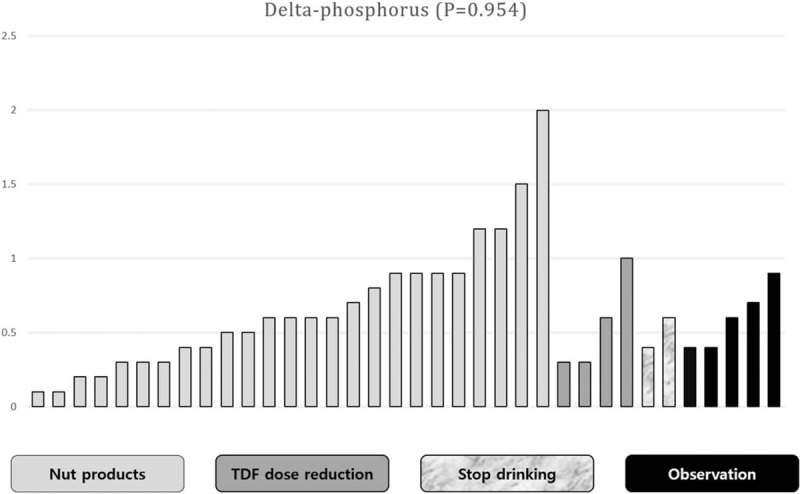
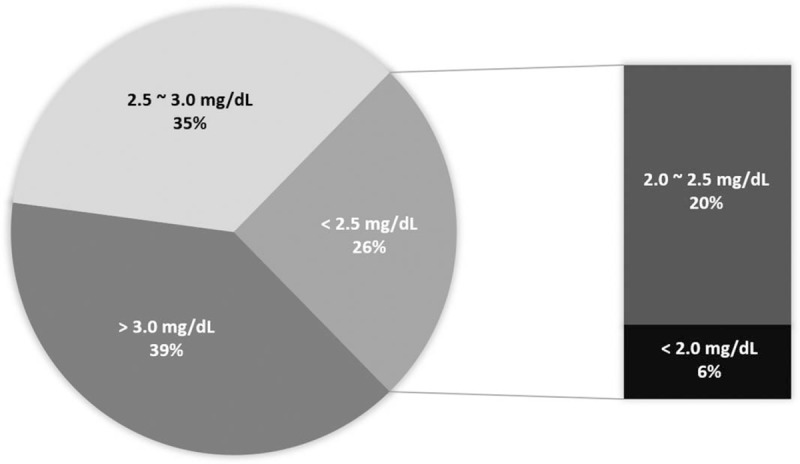
Tenofovir disoproxil fumarate (TDF) is thought to cause varying degrees of hypophosphatemia in patients with chronic hepatitis B (CHB). Therefore, we investigated factors that cause hypophosphatemia in patients treated with TDF and methods to increase serum phosphorus concentrations in clinical practice.We completed a retrospective review of patients with CHB treated with TDF initially at Kosin University Gospel Hospital, Busan, Korea from January 2012 to January 2017. Subclinical hypophosphatemia and hypophosphatemia were defined as serum phosphorus below 3.0 mg/dL and 2.5 mg/dL, respectively.We screened 206 patients with CHB treated with TDF, among which 135 were excluded for the following reasons: baseline malignancy (59), limited data (50), co-administered other antivirals (14), hypophosphatemia at baseline (7), and other reasons (5). The final study population comprised 71 patients. Subclinical hypophosphatemia developed in 43 (60.5%) patients. Hypophosphatemia occurred in 18 patients (25.3%). Liver cirrhosis was the most significant predictor of hypophosphatemia (P = .038, OR = 3.440, CI = 1.082-10.937) Patients diagnosed with subclinical hypophosphatemia were encouraged to increase their intake of nuts and dairy products (25 patients) or reduce their alcohol intake (2), dose reduction of TDF (4) or placed under observation (4). Among patients with subclinical hypophosphatemia, serum phosphorus concentrations were elevated (>3.0 mg/dL) in 23 of 36 patients (63.8%). Increased nut and dairy intake increased phosphorus concentrations to more than 3.0 mg/dl in 16 of 25 patients (64.0%).Entecavir or tenofovir alafenamide fumarate (TAF) should be considered rather than TDF in patients with liver cirrhosis because of the risk of hypophosphatemia. Instead of stopping TDF treatment, encouraging increased intake of phosphorus-rich foods could increase serum phosphorus concentrations in clinical practice.
富马酸替诺福韦二吡呋酯(TDF)被认为会导致慢性乙型肝炎(CHB)患者出现不同程度的低磷血症。因此,我们在临床实践中研究了TDF治疗患者发生低磷血症的相关因素以及提高血清磷浓度的方法。我们对2012年1月至2017年1月在韩国釜山光州大学福音医院初治TDF的CHB患者进行了回顾性研究。亚临床低磷血症和低磷血症分别定义为血清磷低于3.0mg/dL和2.5mg/dL。我们筛选了206例接受TDF治疗的CHB患者,其中135例因以下原因被排除:基线恶性肿瘤(59例)、数据有限(50例)、联合使用其他抗病毒药物(14例)、基线低磷血症(7例)及其他原因(5例)。最终研究人群包括71例患者。43例(60.5%)患者出现亚临床低磷血症。18例(25.3%)患者发生低磷血症。肝硬化是低磷血症最显著的预测因素(P = 0.038,OR = 3.440,CI = 1.082 - 10.937)。对于诊断为亚临床低磷血症的患者,鼓励增加坚果和乳制品摄入量(25例)或减少酒精摄入量(2例)、减少TDF剂量(4例)或进行观察(4例)。在亚临床低磷血症患者中,36例患者中有23例(63.8%)血清磷浓度升高(>3.0mg/dL)。25例患者中有16例(64.0%)通过增加坚果和乳制品摄入量使磷浓度升高至3.0mg/dl以上。由于存在低磷血症风险,对于肝硬化患者应考虑使用恩替卡韦或富马酸替诺福韦艾拉酚胺(TAF)而非TDF。在临床实践中,与其停止TDF治疗,鼓励增加富含磷食物的摄入量可提高血清磷浓度。