Section of Allergy and Immunology, Food Challenge and Research Unit, Children's Hospital Colorado, University of Colorado School of Medicine, Aurora.
Section of Allergy and Immunology, Dartmouth-Hitchcock Medical Center, Lebanon, New Hampshire.
JAMA Netw Open. 2019 Dec 2;2(12):e1918041. doi: 10.1001/jamanetworkopen.2019.18041.
Early peanut introduction reduces the risk of developing peanut allergy, especially in high-risk infants. Current US recommendations endorse screening but are not cost-effective relative to other international strategies.
To identify scenarios in which current early peanut introduction guidelines would be cost-effective.
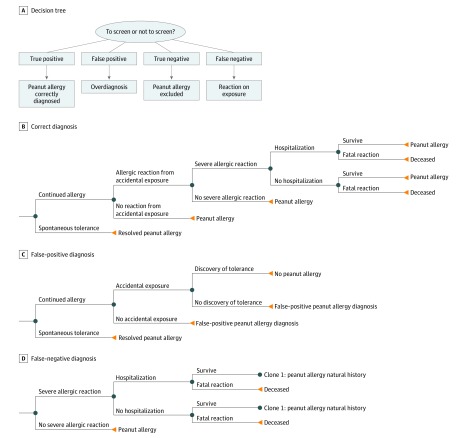
DESIGN, SETTING, AND PARTICIPANTS: This simulation/cohort economic evaluation used microsimulations and cohort analyses in a Markov model to evaluate the cost-effectiveness of early peanut introduction with and without peanut skin prick test (SPT) screening in high-risk infants during an 80-year horizon from a societal perspective. Data were analyzed from April to May 2019.
High-risk infants with early-onset eczema and/or egg allergy underwent early peanut introduction with and without peanut SPT screening (100 000 infants per treatment strategy) using a dichotomous 8-mm SPT cutoff value (stipulated in the current US guideline).
Cost, quality-adjusted life-years (QALYs), net monetary benefit, peanut allergic reactions, severe allergic reactions, and deaths due to peanut allergy.
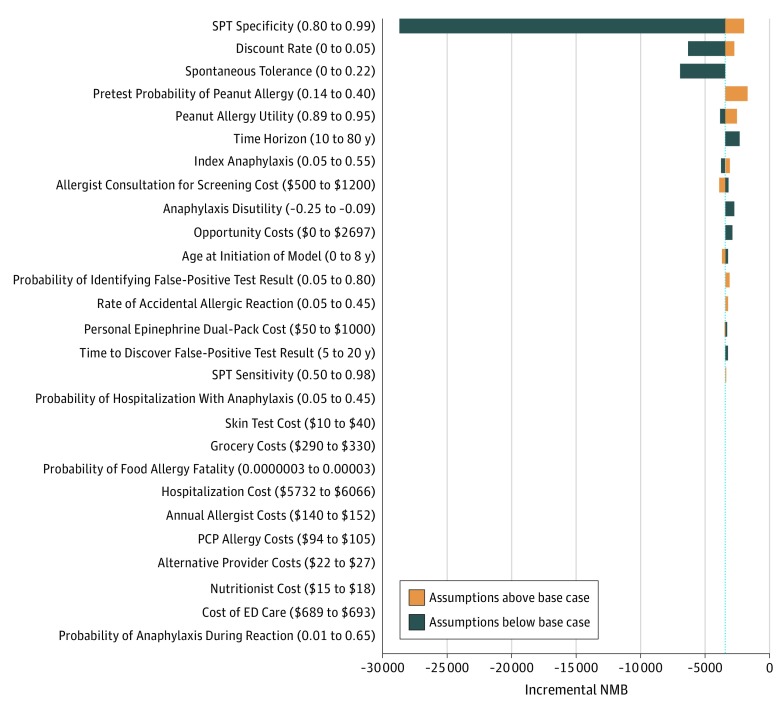
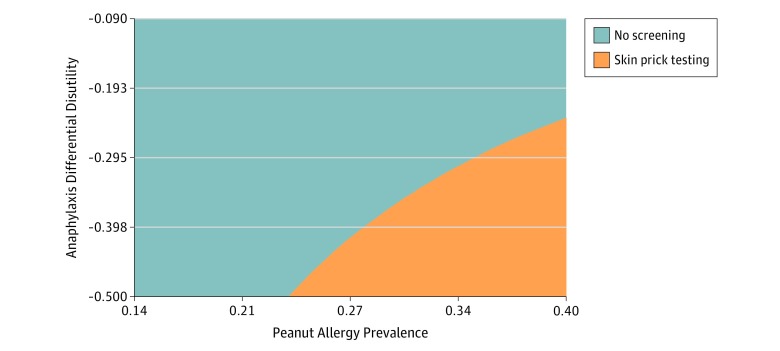
In the simulated cohort of 200 000 infants and using the base case during the model horizon, a no-screening approach had lower mean (SD) costs ($13 449 [$38 163] vs $15 279 [$38 995]) and higher mean (SD) gain in QALYs (29.25 [3.28] vs 29.23 [3.30]) vs screening but resulted in more allergic reactions (mean [SD], 1.07 [3.15] vs 1.01 [3.02]), severe allergic reactions (mean [SD], 0.53 [1.66] vs 0.52 [1.62]), and anaphylaxis involving cardiorespiratory compromise (mean [SD], 0.50 [1.59] vs 0.49 [1.47]) per individual. In deterministic SPT sensitivity analyses at base-case sensitivity and specificity rates, screening could be cost-effective at a high disutility rate (the negative effect of a food allergic reaction) (76-148 days of life traded) for an at-home vs in-clinic reaction in combination with high baseline peanut allergy prevalence among infants at high risk for peanut allergy and not yet exposed to peanuts. If an equivalent rate and disutility of accidental and index anaphylaxis was assumed and the 8-mm SPT cutoff had 0.85 sensitivity and 0.98 specificity, screening was cost-effective at a peanut allergy prevalence of 36%.
The results of this study suggest that the current screening approach to early peanut introduction could be cost-effective at a particular health utility for an in-clinic reaction, SPT sensitivity and specificity, and high baseline peanut allergy prevalence among high-risk infants. However, such conditions are unlikely to be plausible to realistically achieve. Further research is needed to define the health state utility associated with reaction location.
早期引入花生可降低发生花生过敏的风险,尤其是对高危婴儿。目前美国的建议支持进行筛查,但相对于其他国际策略而言,其成本效益并不高。
确定目前早期引入花生的指南在哪些情况下具有成本效益。
设计、设置和参与者:本仿真/队列经济学评估使用微仿真和队列分析在马尔可夫模型中,从社会角度评估了在 80 年的时间内,对高风险婴儿进行早期花生引入(有无花生皮试(SPT)筛查)的成本效益,高危婴儿伴有早发性特应性皮炎和/或鸡蛋过敏。使用 8 毫米 SPT 截断值(当前美国指南中规定的)对 100000 名婴儿进行每一种治疗策略的 SPT 筛查。
有早发性特应性皮炎和/或鸡蛋过敏的高危婴儿接受早期花生引入(有无花生 SPT 筛查)。使用 8 毫米 SPT 截断值(当前美国指南中规定的)对 100000 名婴儿进行每一种治疗策略的 SPT 筛查。
成本、质量调整生命年(QALY)、净货币收益、花生过敏反应、严重过敏反应和因花生过敏导致的死亡。
在模型预测期间的 200000 名婴儿模拟队列中,在使用基础案例的情况下,不筛查方法的平均(标准差)成本较低(13449 美元[38163 美元]与 15279 美元[38995 美元]),平均(标准差)QALY 增益较高(29.25[3.28]与 29.23[3.30]),但筛查结果导致更多过敏反应(平均[标准差],1.07[3.15]与 1.01[3.02])、严重过敏反应(平均[标准差],0.53[1.66]与 0.52[1.62])和涉及心肺功能受损的过敏反应(平均[标准差],0.50[1.59]与 0.49[1.47])。在基于基础案例敏感性和特异性的 SPT 敏感性分析中,如果在门诊反应中使用高不适率(食物过敏反应的负面影响)(76-148 天的生命换取)和高基线花生过敏在高风险花生过敏婴儿中流行率(尚未接触过花生)进行家庭与门诊反应的比较,那么筛查可能具有成本效益。如果假设意外和索引过敏反应的等效率和不适率,且 8 毫米 SPT 截断值具有 0.85 的敏感性和 0.98 的特异性,那么在花生过敏流行率为 36%的情况下,筛查具有成本效益。
本研究结果表明,目前对早期花生引入的筛查方法可能在特定的健康效用、门诊反应的 SPT 敏感性和特异性以及高风险婴儿的高基线花生过敏流行率方面具有成本效益。然而,这些情况不太可能是现实的。需要进一步研究来确定与反应位置相关的健康状态效用。