Gilead Sciences, Inc, Foster City, CA, USA.
San Francisco Department of Public Health, San Francisco, CA, USA.
J Int AIDS Soc. 2019 Dec;22(12):e25433. doi: 10.1002/jia2.25433.
New HIV diagnoses have fallen in the past decade due to increased HIV testing, earlier diagnosis, earlier antiretroviral treatment, improved linkage to care and engagement in care, and the recent increased uptake of pre-exposure prophylaxis (PrEP). We propose a novel method to compute the rate of new HIV diagnoses at the Metropolitan Statistical Area (MSA) level in the US to support the evaluation of comprehensive treatment and prevention efforts over time.
The number of new HIV diagnoses, number of individuals with a PrEP indication and aggregated person-time exposed to PrEP during the years 2012 to 2017 were used to compute a new HIV diagnosis rate for people at risk of HIV excluding those already on PrEP for the 105 MSAs in the US with published HIV surveillance data. In our calculation of person-time with a PrEP indication, time-at-risk excluded time on PrEP and time after an HIV diagnosis. We used a multivariate Poisson regression model to estimate HIV diagnosis rates by year and location.
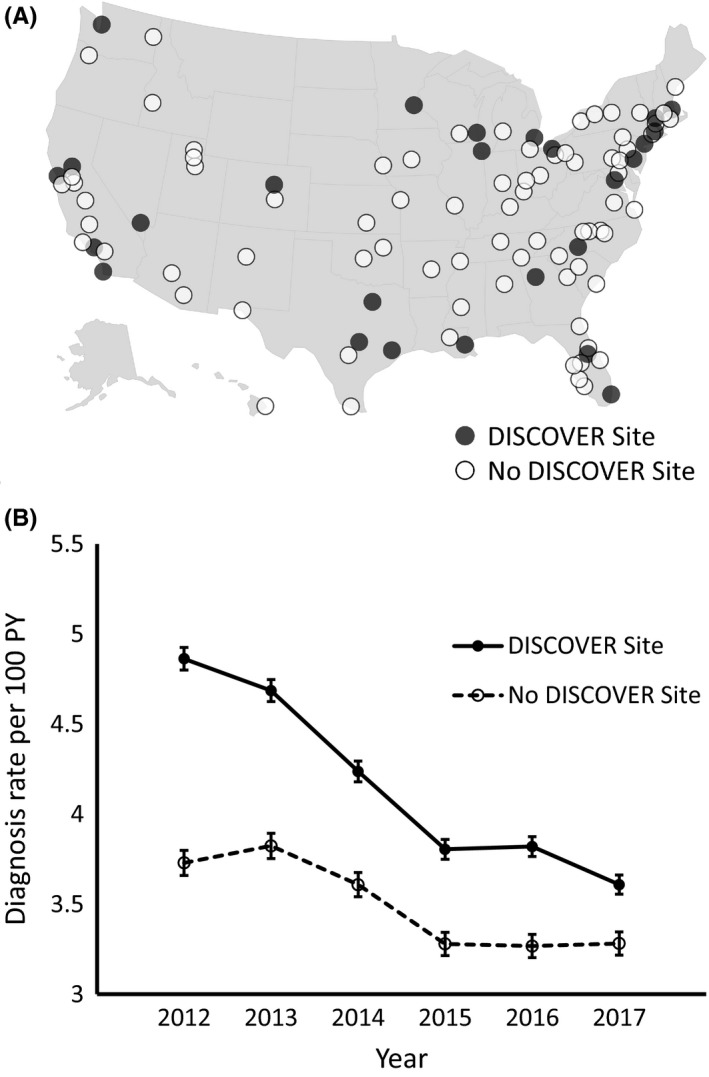
From 2012 to 2017, the aggregate HIV diagnoses rate among high-risk individuals with an indication for PrEP in the 105 MSAs decreased from 4.14 per 100 person-years (PY) (95% CI 4.10 to 4.19) to 3.26 per 100 PY (95% CI 3.22 to 3.30). For the 25 US MSAs that overlapped with an ongoing large randomized clinical trial of PrEP in men who have sex with men (MSM), the HIV diagnosis rate from 2012 to 2017 decreased from 4.86 per 100 PY (95% CI 4.80 to 4.93) to 3.61 per 100 PY (95% CI 3.56 to 3.66), a decline that was more rapid than in non-study MSAs (IRR for trial site 1.19, 95% CI 1.18 to 1.20).
We propose a model to estimate the background HIV diagnosis rate in people at risk for HIV and with a PrEP indication in US MSAs (excluding those on PrEP) using publically available surveillance data which can evaluate trends over time. Data generated using this methodology could be used by policy makers and local HIV prevention specialists to evaluate and monitor their prevention efforts for the population at risk in their communities.
由于 HIV 检测的增加、早期诊断、早期抗逆转录病毒治疗、改善与护理的联系以及最近接受暴露前预防 (PrEP) 的人数增加,过去十年中 HIV 的新诊断病例有所下降。我们提出了一种新的方法,以便在美国大都市统计区 (MSA) 层面计算新的 HIV 诊断率,以支持随着时间的推移评估综合治疗和预防工作的效果。
利用 2012 年至 2017 年期间新的 HIV 诊断数量、有 PrEP 指征的人数和聚合的 PrEP 暴露人数,为美国 105 个具有已发表 HIV 监测数据的 MSA 中处于 HIV 风险中的人群(不包括已经接受 PrEP 的人群)计算新的 HIV 诊断率。在计算有 PrEP 指征的人时,我们将风险时间排除了 PrEP 时间和 HIV 诊断后的时间。我们使用多变量泊松回归模型按年和地点估计 HIV 诊断率。
2012 年至 2017 年,105 个 MSA 中高危人群中 PrEP 指征人群的 HIV 综合诊断率从每 100 人年 4.14 例(95%置信区间 4.10 至 4.19)下降到每 100 人年 3.26 例(95%置信区间 3.22 至 3.30)。对于 25 个与正在进行的男男性行为人群中 PrEP 大型随机临床试验重叠的美国 MSA,2012 年至 2017 年 HIV 诊断率从每 100 人年 4.86 例(95%置信区间 4.80 至 4.93)下降到每 100 人年 3.61 例(95%置信区间 3.56 至 3.66),下降速度快于非研究 MSA(试验地点的发病率比为 1.19,95%置信区间为 1.18 至 1.20)。
我们提出了一种使用公共监测数据来估计美国 MSA 中处于 HIV 风险中且有 PrEP 指征的人群(不包括接受 PrEP 的人群)的背景 HIV 诊断率的模型,该模型可以随时间评估趋势。使用这种方法生成的数据可由政策制定者和当地 HIV 预防专家用于评估和监测其社区内高危人群的预防工作。