Bierhoff M, Pinyopornpanish Kanokporn, Pinyopornpanish Kanokwan, Tongprasert F, Keereevijit Arunrot, Rijken M, Chu C S, Nosten F, Perfetto J, van Vugt M, Mcgready R, Angkurawaranon C
Shoklo Malaria Research Unit, Mahidol-Oxford Tropical Medicine Research Unit, Mahidol University, Mae Sot, Thailand.
Division of Infectious Diseases, Academic Medical Center, University of Amsterdam, Amsterdam, The Netherlands.
Open Forum Infect Dis. 2019 Dec 7;6(12):ofz518. doi: 10.1093/ofid/ofz518. eCollection 2019 Dec.
Vaccination remains the mainstay of prevention of hepatitis B virus (HBV) including birth dose and hepatitis B immunoglobulins (HBIGs). National estimates of vaccination coverage exclude migrants. The objective of this study is to investigate documentation practices of HBV-related infant vaccinations in Northern Thailand including migrants.
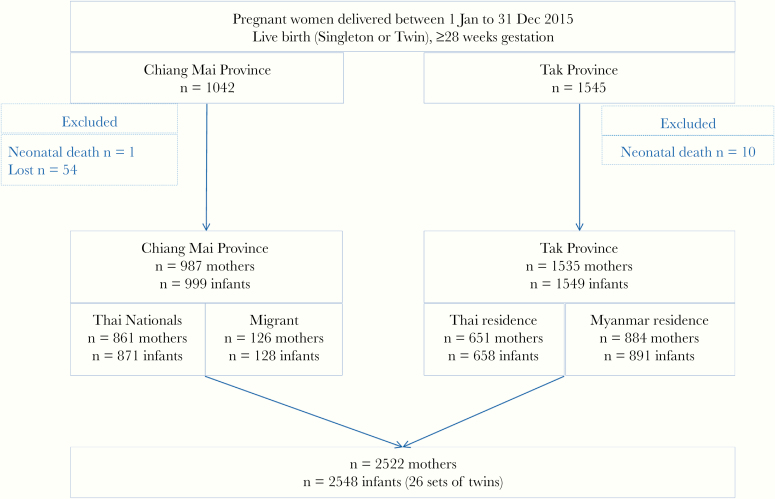
This is a retrospective review of hospital records of women who birthed infants in 2015 at Maharaj Nakorn Hospital, Chiang Mai (CM) or on the Thailand-Myanmar border, Tak.
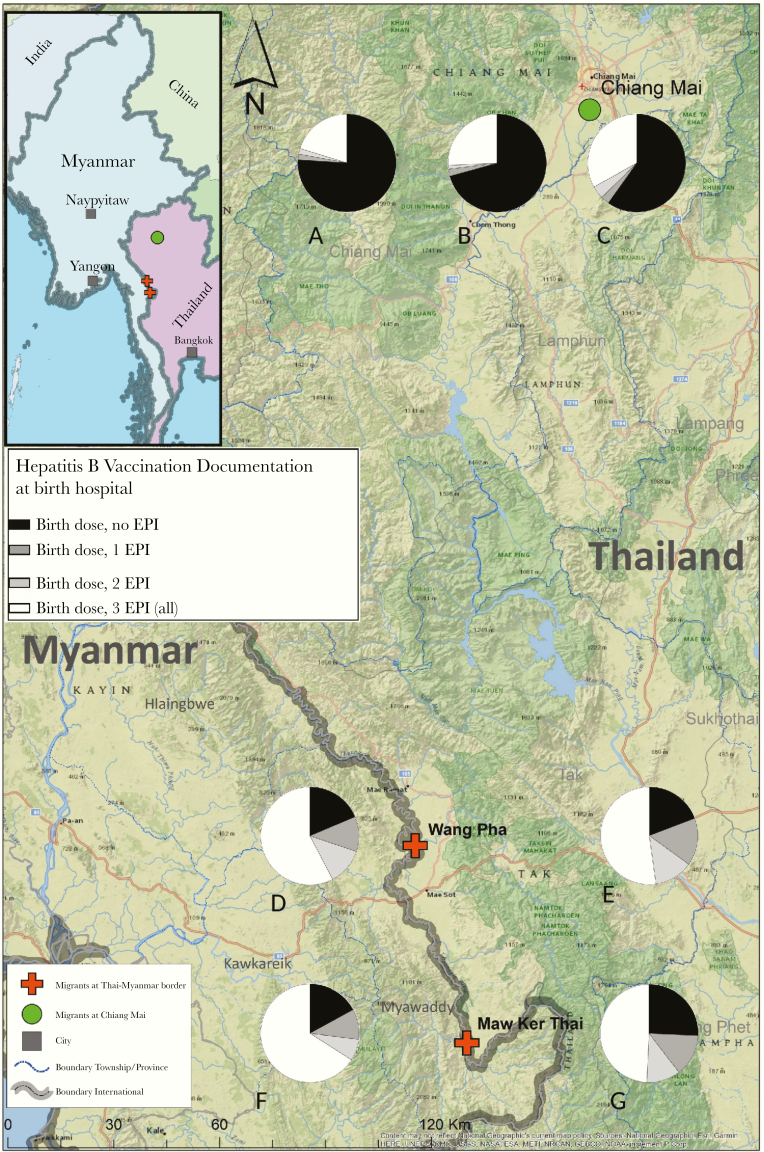
Of 2522 women, 987 were from CM (861 Thai nationals, 126 migrants) and 1535 were from Tak (651 Thai residence and 884 Myanmar residence). In CM, documentation for the birth dose vaccine (999 of 999, 100%) and HBIG was complete. In Tak, documentation was 1441 of 1549 (93%) for birth dose and 26 of 34 (76.5%) for HBIG, with missed opportunities including home delivery, delay in obtaining hepatitis B e-antigen status, and limitations of the records. Expanded Program of Immunization (EPI) documentation of 3 follow-up vaccinations dwindled with subsequent doses and distance, and complete documentation of 3 HBV EPI vaccines at the hospital of birth was low, 41.5% (1056 of 2547), but equitable for Thai or migrant status.
This review provides strong support for excellent documentation of HBIG and birth dose vaccination in urban and rural settings, and in migrants, consistent with Thailand's vaccination policy and practice. Documentation of the 3 HBV EPI at the hospital of birth decreases with sequential doses, especially in families further away. Innovative data linkage is required to prove coverage and identify gaps.
接种疫苗仍然是预防乙型肝炎病毒(HBV)的主要手段,包括出生剂量疫苗和乙型肝炎免疫球蛋白(HBIG)。全国疫苗接种覆盖率的估计不包括移民。本研究的目的是调查泰国北部包括移民在内的与HBV相关的婴儿疫苗接种记录情况。
这是一项对2015年在清迈的玛哈拉吉·那空医院(CM)或泰国-缅甸边境的达府分娩婴儿的妇女的医院记录进行的回顾性研究。
在2522名妇女中,987名来自CM(861名泰国国民,126名移民),1535名来自达府(651名泰国居民和884名缅甸居民)。在CM,出生剂量疫苗(999例中的999例,100%)和HBIG的记录完整。在达府,出生剂量疫苗的记录为1549例中的1441例(93%),HBIG的记录为34例中的26例(76.5%),错过记录的情况包括在家分娩、获取乙肝e抗原状态延迟以及记录的局限性。3次后续疫苗接种的扩大免疫规划(EPI)记录随着后续剂量和距离的增加而减少,在出生医院3次HBV EPI疫苗的完整记录率较低,为41.5%(2547例中的1056例),但泰国人或移民身份的记录情况相当。
本综述有力支持了在城市和农村地区以及移民中对HBIG和出生剂量疫苗接种进行良好记录,这与泰国的疫苗接种政策和实践一致。出生医院3次HBV EPI疫苗的记录随着接种剂量的增加而减少,尤其是在距离较远的家庭中。需要创新的数据关联来证明覆盖率并找出差距。