Shoklo Malaria Research Unit, Mahidol-Oxford Tropical Medicine Research Unit, Mahidol University, Mae Sot, 63110, Thailand.
Division of Infectious Diseases, Academic Medical Center, University of Amsterdam, Amsterdam, The Netherlands.
BMC Pregnancy Childbirth. 2021 Feb 22;21(1):157. doi: 10.1186/s12884-021-03612-z.
Hepatitis B Virus (HBV) is transmitted from mother to child which can be prevented via birth dose vaccine combined with three follow up hepatitis B vaccines, hepatitis B immunoglobulins (HBIG), and maternal antiviral treatment with Tenofovir Disoproxil Fumarate (TDF). This study evaluates the cost effectiveness of six strategies to prevent perinatal HBV transmission in a resource limited setting (RLS) on the Thailand-Myanmar border.
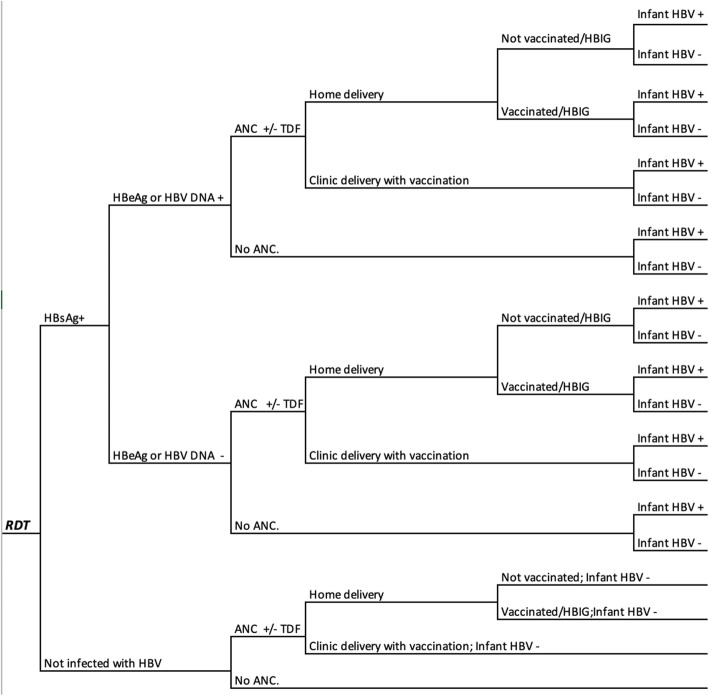
The cost effectiveness of six strategies was tested by a decision tree model in R. All strategies included birth and follow up vaccinations and compared cost per infection averted against two willingness to pay thresholds: one-half and one gross domestic product (GDP) per capita. Strategies were: 1) Vaccine only, 2) HBIG after rapid diagnostic test (RDT): infants born to HBsAg+ are given HBIG, 3) TDF after RDT: HBsAg+ women are given TDF, 4) TDF after HBeAg test: HBeAg+ women are given TDF, 5) TDF after high HBV DNA: women with HBV DNA > 200,000 are given TDF, 6) HBIG & TDF after high HBV DNA: women with HBV DNA > 200,000 are given TDF and their infants are given HBIG. One-way and probabilistic sensitivity analyses were conducted on the cost-effective strategies.
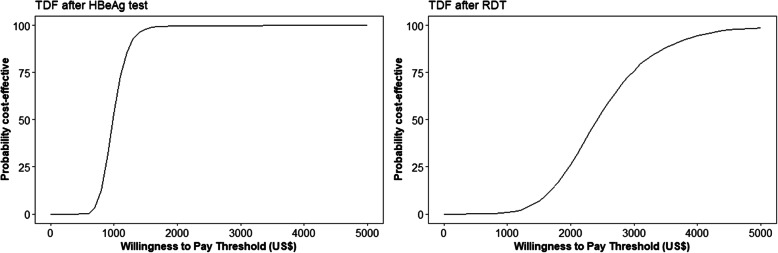
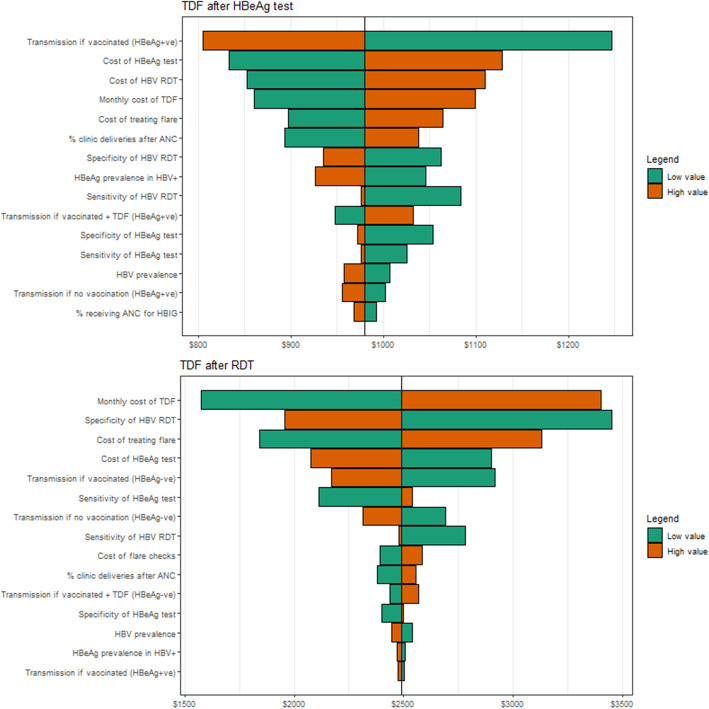
Vaccine only was the least costly option with TDF after HBeAg test strategy as the only cost-effective alternative. TDF after HBeAg test had an incremental cost-effectiveness ratio of US$1062; which would not be considered cost-effective with the lower threshold of one-half GDP per capita. The one-way sensitivity analysis demonstrated that the results were reasonably robust to changes in single parameter values. The PSA showed that TDF after HBeAg test had an 84% likelihood of being cost effective at a willingness to pay threshold of one GDP per capita per infection averted.
We found that TDF after HBeAg test has the potential to be cost-effective if TDF proves effective locally to prevent perinatal HBV transmission. The cost of TDF treatment and reliability of the RDT could be barriers to implementing this strategy. While TDF after RDT may be a more feasible strategy to implement in RLS, TDF after HBeAg test is a less costly option.
乙型肝炎病毒(HBV)可通过母婴传播,通过在出生时接种疫苗,并结合后续三次乙肝疫苗、乙肝免疫球蛋白(HBIG)以及替诺福韦二吡呋酯(TDF)的母亲抗病毒治疗,可以预防母婴传播。本研究评估了在泰国-缅甸边境资源有限环境(RLS)下,预防围产期 HBV 传播的六种策略的成本效益。
通过决策树模型在 R 语言中测试了六种策略的成本效益。所有策略均包括出生时和后续的疫苗接种,并比较了每例感染预防的成本与两个意愿支付阈值:一半和一个人均国内生产总值(GDP)。策略如下:1)仅疫苗,2)快速诊断检测(RDT)后 HBIG:HBsAg+ 婴儿出生时给予 HBIG,3)RDT 后 TDF:HBsAg+ 女性给予 TDF,4)HBeAg 检测后 TDF:HBeAg+ 女性给予 TDF,5)高 HBV DNA 后 TDF:HBV DNA>200,000 的女性给予 TDF,6)高 HBV DNA 后 HBIG 和 TDF:HBV DNA>200,000 的女性给予 TDF,其婴儿给予 HBIG。对成本效益策略进行了单因素和概率敏感性分析。
仅疫苗是最具成本效益的选择,而 HBeAg 检测后 TDF 策略是唯一具有成本效益的替代方案。HBeAg 检测后 TDF 的增量成本效益比为 1062 美元;如果以低于一半人均 GDP 的阈值计算,这将不是一个具有成本效益的选择。单因素敏感性分析表明,结果对单个参数值的变化具有较强的稳健性。PSA 表明,如果 TDF 在当地被证明有效以预防围产期 HBV 传播,HBeAg 检测后 TDF 有 84%的可能性在一个人均 GDP 每例感染预防的意愿支付阈值下具有成本效益。
我们发现,如果 TDF 被证明能有效预防围产期 HBV 传播,HBeAg 检测后 TDF 具有成为成本效益的潜力。TDF 治疗的成本和 RDT 的可靠性可能是实施这一策略的障碍。虽然 RDT 后 TDF 可能是 RLS 中更可行的实施策略,但 HBeAg 检测后 TDF 是一种成本更低的选择。