Chen Ellie, Abu-Sbeih Hamzah, Thirumurthi Selvi, Mallepally Niharika, Khurana Shruti, Wei Dongguang, Altan Mehmet, Morris Van K, Tan Dongfeng, Barcenas Carlos H, Wang Yinghong
Department of Medicine, Baylor College of Medicine (Ellie Chen, Niharika Mallepally).
Department of Gastroenterology, Hepatology and Nutrition, The University of Texas MD Anderson Cancer Center (Hamzah Abu-Sbeih, Selvi Thirumurthi, Yinghong Wang).
Ann Gastroenterol. 2020 Jan-Feb;33(1):59-67. doi: 10.20524/aog.2019.0431. Epub 2019 Nov 21.
Limited data are available concerning the clinical features of toxic gastrointestinal (GI) effects of taxane-based therapy. We describe the clinical, endoscopic and histologic features of taxane-induced colitis.
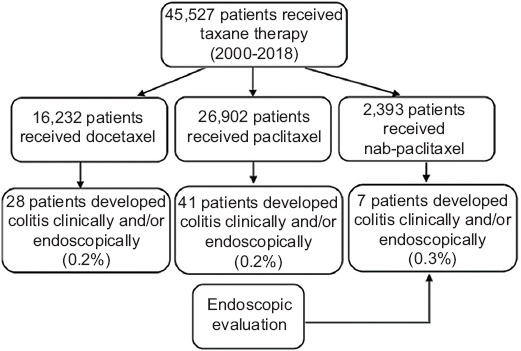
This retrospective study included cancer patients who received taxane therapy and underwent colonoscopy for GI symptoms from 2000-2018.
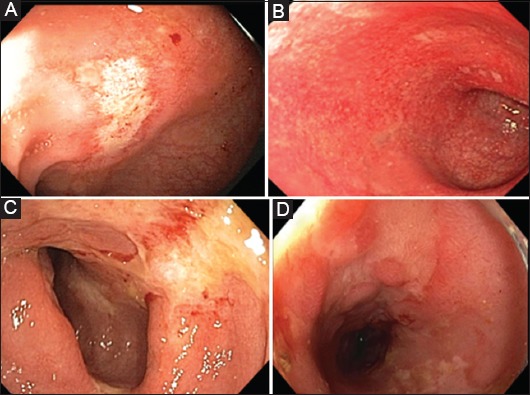
Of the 45,527 patients who received taxane therapy during the study period, 76 (0.2%) met the inclusion criteria. Most patients (54%) received paclitaxel, 37% docetaxel, and 9% nab-paclitaxel. The median time from taxane therapy initiation to colitis symptom onset was 31 days. The median duration of colitis symptoms was 30 days. Colitis treatment comprised immunosuppressive therapy in 8 patients (11%), antibiotics in 17 (22%), antimotility agents in 18 (24%), and octreotide or somatostatin in 2 (3%). Thirty-five patients (46%) required hospitalization and seven (9%) required admission to the intensive care unit (ICU). Endoscopy revealed mucosal ulceration in 19 patients (25%), nonulcerative inflammation in 32 (42%), and normal findings in 25 (33%). Seventeen patients (22%) had features of lymphocytic colitis. One patient had spontaneous colonic perforation that required surgical intervention. Colitis symptoms recurred in 7 patients (9%) after initial improvement. Patients who received nab-paclitaxel developed GI toxicity earlier (P=0.003), required colitis-related hospitalization more frequently (P=0.005), and received intravenous fluids more frequently (P=0.025), compared with patients who received other taxanes.
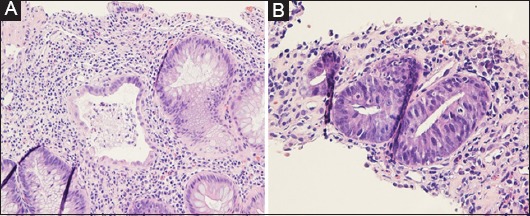
Taxane-related colitis can present with significant inflammation on colonoscopy, and in a minority of patients as microscopic colitis. Taxane-induced colitis, although uncommon, can lead to ICU admission and colonic perforation.
关于紫杉烷类疗法引起的胃肠道毒性作用的临床特征,现有数据有限。我们描述了紫杉烷诱导的结肠炎的临床、内镜和组织学特征。
这项回顾性研究纳入了2000年至2018年间接受紫杉烷类疗法并因胃肠道症状接受结肠镜检查的癌症患者。
在研究期间接受紫杉烷类疗法的45527例患者中,76例(0.2%)符合纳入标准。大多数患者(54%)接受紫杉醇治疗,37%接受多西他赛治疗,9%接受白蛋白结合型紫杉醇治疗。从开始紫杉烷类疗法到出现结肠炎症状的中位时间为31天。结肠炎症状的中位持续时间为30天。结肠炎治疗包括8例患者(11%)接受免疫抑制治疗,17例(22%)接受抗生素治疗,18例(24%)接受止泻药治疗,2例(3%)接受奥曲肽或生长抑素治疗。35例患者(46%)需要住院治疗,7例(9%)需要入住重症监护病房(ICU)。内镜检查显示,19例患者(25%)有黏膜溃疡,32例(42%)有非溃疡性炎症,25例(33%)检查结果正常。17例患者(22%)有淋巴细胞性结肠炎的特征。1例患者发生自发性结肠穿孔,需要手术干预。7例患者(9%)在最初病情改善后结肠炎症状复发。与接受其他紫杉烷类药物的患者相比,接受白蛋白结合型紫杉醇治疗的患者更早出现胃肠道毒性(P=0.003),更频繁地因结肠炎住院(P=0.005),更频繁地接受静脉补液(P=0.025)。
紫杉烷相关的结肠炎在结肠镜检查时可表现为明显炎症,少数患者表现为显微镜下结肠炎。紫杉烷诱导的结肠炎虽然不常见,但可导致入住ICU和结肠穿孔。