Messina Francesco, Clavenna Antonio, Cartabia Massimo, Piovani Daniele, Bortolotti Angela, Fortino Ida, Merlino Luca, Bonati Maurizio
Laboratory for Mother and Child Health, Department of Public Health, Istituto di Ricerche Farmacologiche Mario Negri IRCCS, Milano, Italy.
Regional Health Ministry, Lombardy Region, Milan, Italy.
BMJ Paediatr Open. 2019 Dec 11;3(1):e000546. doi: 10.1136/bmjpo-2019-000546. eCollection 2019.
This study aimed to assess the appropriateness of antibiotic prescription in children seen in emergency departments (EDs) and to compare prescription profiles in ED and primary care.
This is a retrospective analysis of healthcare administrative databases.
The study analysed data collected in emergency departments (EDs) and primary care practices (PCPs) in Lombardy, Italy.
Children and adolescents between 1 and 13 years old with an ED access and/or an antibiotic prescription in the first semester of 2012 participated in the study. Only those with an index event (ie, without ED access, hospital admissions or antibiotic prescriptions in the previous 60 days) were included.
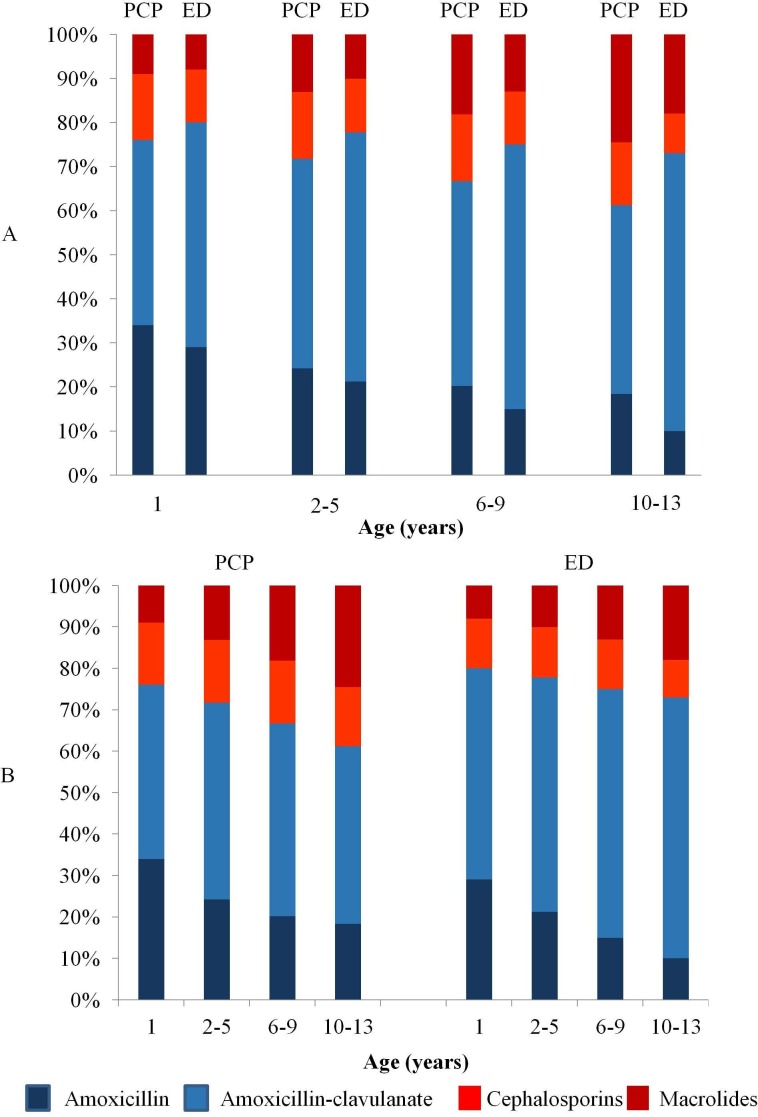
The main outcomes are percentage of subjects receiving amoxicillin (first-choice antibiotic) and percentages receiving macrolides/cephalosporins (second-choice therapies).
During the observation period, 133 275 children had one ED access, and 26 087 (19.6%) received an antibiotic prescription. In all, 56.1% of children seen for upper respiratory tract infections (URTIs) received an antibiotic, with a prevalence of 67.8% for otitis media and 56.4% for pharyngotonsillitis; 22.3% of children were given amoxicillin after a visit for URTIs, with no differences among infections, and 19.6% received macrolides and cephalosporins. Few differences were found when comparing the index antibiotic prescriptions in ED and PCP settings. A higher prescription of second-choice antibiotics was observed among children cared for by PCPs compared with children attending EDs (31.3% vs 23.4%, χ =720, p<0.001). The place of residence was the main determinant of the qualitative profile of prescriptions.
More must be done to improve rational use of antibiotics in the ED and PCP setting, and educational interventions including physicians in both setting are strongly needed.
本研究旨在评估急诊科就诊儿童抗生素处方的合理性,并比较急诊科与初级保健机构的处方情况。
这是一项对医疗管理数据库的回顾性分析。
该研究分析了意大利伦巴第地区急诊科和初级保健机构收集的数据。
2012年上半年有急诊科就诊记录和/或抗生素处方的1至13岁儿童及青少年参与了本研究。仅纳入那些有索引事件的患者(即过去60天内无急诊科就诊、住院或抗生素处方)。
主要观察指标为接受阿莫西林(首选抗生素)治疗的受试者百分比以及接受大环内酯类/头孢菌素类(次选治疗药物)治疗的百分比。
在观察期内,133275名儿童有一次急诊科就诊记录,其中26087名(19.6%)接受了抗生素处方。总体而言,因上呼吸道感染(URTIs)就诊的儿童中有56.1%接受了抗生素治疗,中耳炎的患病率为67.8%,咽扁桃体炎的患病率为56.4%;因URTIs就诊后,22.3%的儿童使用了阿莫西林,不同感染类型之间无差异,19.6%的儿童接受了大环内酯类和头孢菌素类治疗。比较急诊科和初级保健机构的索引抗生素处方时,发现差异不大。与在急诊科就诊的儿童相比,初级保健机构照料的儿童中次选抗生素的处方率更高(31.3%对23.4%,χ =720,p<0.001)。居住地点是处方质量特征的主要决定因素。
必须采取更多措施以改善急诊科和初级保健机构抗生素的合理使用,强烈需要对包括这两个机构的医生在内进行教育干预。