Health Technology Assessment, Department of Epidemiology, University of Groningen, University Medical Centre Groningen, Groningen, The Netherlands
Health Technology Assessment, Department of Epidemiology, University of Groningen, University Medical Centre Groningen, Groningen, The Netherlands.
BMJ Open. 2020 Jan 7;10(1):e032754. doi: 10.1136/bmjopen-2019-032754.
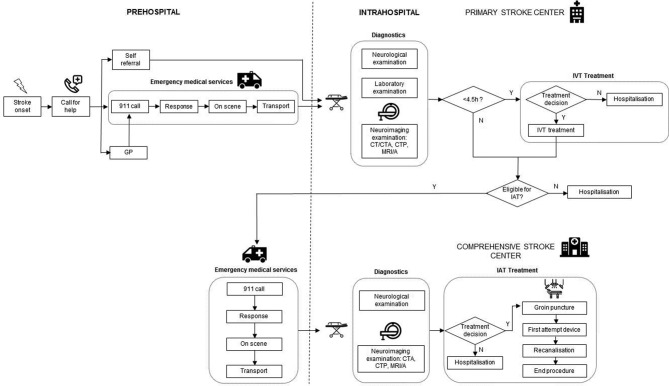
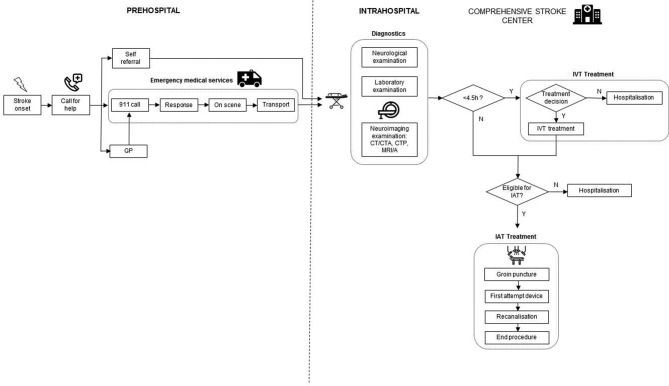
The introduction of intra-arterial thrombectomy (IAT) challenges acute stroke care organisations to provide fast access to acute stroke therapies. Parameters of pathway performance include distances to primary and comprehensive stroke centres (CSCs), time to treatment and availability of ambulance services. Further expansion of IAT centres may increase treatment rates yet could affect efficient use of resources and quality of care due to lower treatment volume. The aim was to study the organisation of care and patient logistics of IAT for patients with ischaemic stroke in the Netherlands.
Using a simulation modelling approach, we will quantify performance of 16 primary and CSCs offering IAT in the Netherlands. Patient data concerning both prehospital and intrahospital pathway logistics will be collected and used as input for model validation. A previously validated simulation model for intravenous thrombolysis (IVT) patients will be expanded with data of the MR CLEAN (Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands) Registry and trials performed in the Collaboration for New Treatments in Acute Stroke consortium to represent patient logistics, time delays and outcomes in IAT patients. Simulation experiments aim to assess effectiveness and efficiency of alternative network topologies, that is, IAT with or without IVT at the nearest primary stroke centre (PSC) versus centralised care at a CSC. Primary outcomes are IAT treatment rates and clinical outcome according to the modified Rankin Scale. Secondary outcomes include onset-to-treatment time and resource use. Mann-Whitney U and Fisher's exact tests will be used to estimate differences for continuous and categorical variables. Model and parameter uncertainty will be tested using sensitivity analyses.
This will be the first study to examine the organisation of acute stroke care for IAT delivery on a national scale using discrete event simulation. There are no ethics or safety concerns regarding the dissemination of information, which includes publication in peer-reviewed journals and (inter)national conference presentations.
ISRCTN99503308, ISRCTN76741621, ISRCTN19922220, ISRCTN80619088, NCT03608423; Pre-results.
动脉内血栓切除术(IAT)的引入使急性脑卒中治疗组织面临提供快速急性脑卒中治疗的挑战。路径性能的参数包括到初级和综合脑卒中中心(CSC)的距离、治疗时间和救护车服务的可用性。进一步扩大 IAT 中心可能会增加治疗率,但由于治疗量较低,可能会影响资源的有效利用和护理质量。目的是研究荷兰缺血性脑卒中患者 IAT 的护理组织和患者物流。
使用模拟建模方法,我们将量化荷兰 16 个提供 IAT 的初级和 CSC 的性能。将收集有关院前和院内通路物流的患者数据,并将其用作模型验证的输入。一个以前经过验证的静脉内溶栓(IVT)患者的模拟模型将扩展到 MR CLEAN(荷兰多中心急性缺血性脑卒中血管内治疗随机临床试验)登记处和协作治疗急性脑卒中联盟进行的试验的数据,以代表 IAT 患者的物流、时间延迟和结果。模拟实验旨在评估替代网络拓扑的有效性和效率,即最近的初级脑卒中中心(PSC)是否进行 IAT 和 IVT 与 CSC 的集中护理。主要结果是 IAT 治疗率和改良 Rankin 量表的临床结果。次要结果包括发病到治疗时间和资源使用。将使用曼-惠特尼 U 检验和 Fisher 确切检验来估计连续和分类变量的差异。将使用敏感性分析来测试模型和参数的不确定性。
这将是第一项使用离散事件模拟在全国范围内检查 IAT 交付的急性脑卒中护理组织的研究。在信息传播方面,没有伦理或安全问题,包括在同行评议的期刊上发表和(国际)会议演示。
ISRCTN80619088,ISRCTN99503308,ISRCTN76741621,ISRCTN19922220,NCT03608423;预结果。